The need for guaranteeing patient safety through error-free services can be understood well only by examining the topic of bar code medication administration (BCMA). This subject introduces to readers and other interested parties technology-based approaches that serve the purpose of minimizing faulty prescriptions by confirming electronically that the health officer has indeed checked various medication administration issues.
This topic has had a substantial impact on nursing care. The BCMA technology influences healthcare delivery by ensuring that physicians serve patients with the recommended dosage and medicine at the proper time using the correct channel of drug prescription. This paper presents an example regarding the application of the bar code medication administration system. It also offers a personal experience whereby the failure of a particular hospital to adopt the BCMA technology led to the death of my workmate.
An Example of Bar Code Medication Administration
In a study by Shah, Lo, Babich, Tsao, and Bansback (2016), BCMA is presented as capable of ensuring that medical practitioners rely on results generated electronically revealing patients’ health history, including prescriptions that should be given to them to enhance their recovery. The functionality of the BCMA may not be understood well without giving an example of how some of its features operate to realize the goal of maintaining patient safety. In particular, this technology has a “Missing Dose Request” feature that enables healthcare providers to monitor the amount and type of drugs available in various wards.
This component recommends the appropriate means of ensuring that tablets, which may be out of stock in particular units, are made accessible to patients, thanks to the existence of a pharmacy that is linked to the BCMA information technology.
The study by Louden et al. (2017) demonstrates how this BCMA feature operates. In particular, a medical officer instigates a Missing Dose Request whereby a pop-out menu opens. Through some computerized printouts, the bar code medication administration framework communicates directly to the chemist requesting the available health officers to release medication doses that are not available in various wards. The pharmacist assesses the applications made before distributing the desired medication to the recommended location within the healthcare facility. This dispensation is made promptly to ensure that no patient misses a drug at the time it is needed.
According to Louden et al. (2017), deploying this BCMA component has been resourceful because it has not only minimized the frequency of calls made by medical practitioners requesting pharmacists to dispatch drugs to some units but also ensured that patients are served with the appropriate medication in the recommended capacity and within the prescribed time. Figure 1 below shows the information relayed to various wards when handling the Missing Dose Request as part of BCMA features.
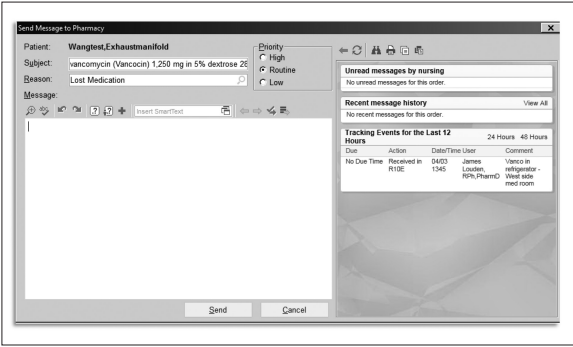
Nonetheless, earlier forms of this feature were linked to various challenges because this software did not include an aspect that could tell the recipient pharmacist the urgency of the request made. As such, much time could pass before any response was made. The implication was that patients who needed emergency services were likely to die following the lack of prompt services. According to Flynn, Evanish, Fernald, Hutchinson, and Lefaiver (2016), an additional feature, namely, the Nursing Medication Order Button, was included to allow the respective medical practitioner to alert the pharmacist that the application made should be documented in the computerized system and dispensed instantaneously.
It is crucial to note that the inclusion of this component made the BCMA technology resourceful when deployed to serve patients who needed emergency services such as those in intensive care units.
Personal Experience
In 2016, an incident happened in my workplace that needed the attention of medical practitioners. In particular, my colleague was involved in an accident whereby he had his legs broken in addition to other major tissue injuries. The dispensation of services within the healthcare facility where he was taken to was not only slow but also non-evidence-based. My colleague lost a huge amount of blood because he could not be provided with the appropriate materials to cover any open wounds at the proper time.
Such elements were not available within the health facility’s emergency department. Ordering the required medication and materials through phone calls and delivering them to the emergency unit took more time because the pharmacist had to first confirm manually the availability of drugs requested instead of checking them electronically and prescribing dosages based on the information developed automatically by the system.
This hospital had not implemented issues raised on the topic of BCMA. My workmate died within three hours after failing to get proper medical services. This situation would have been improved if the hospital had installed the BCMA technology. Having this tool would have enabled pharmacists to dispense the required medications instantaneously while at the same time confirming that indeed the appropriate patient had received the correct amount of the prescribed dosages within the suitable time. It would have eliminated delays brought about by the manual verification of the available drugs.
Conclusion
Today’s healthcare facilities cannot operate optimally without deploying information systems technologies, which not only enhance the quality of services delivered and patients’ safety but also reduce the amount of time spent addressing complicated ailments. Many cases of death have been reported among patients because of medication errors, which could otherwise be avoided by using up-to-date mechanisms such as the bar code medication administration system. In this paper, it has been revealed that the inclusion of the Missing Dose Request and the Nursing Medication Order Button as BCMA features has allowed physicians to give prompt and accurate prescriptions, thus minimizing the number of deaths reported in various healthcare facilities.
References
Flynn, F., Evanish, J., Fernald, J., Hutchinson, D., & Lefaiver, C. (2016). Progressive care nurses improving patient safety by limiting interruptions during medication administration. Critical Care Nurse, 36(4), 19-35.
Louden, L., Mirtallo, J., Worley, M., Naseman, R., Hafford, A., & Brown, N. (2017). Efficiency analysis of a barcode-enabled and integrated medication-tracking system. American Journal of Health-System Pharmacy, 74(23 supplement 4), S84-S89.
Shah, K., Lo, C., Babich, M., Tsao, N., & Bansback, N. (2016). Bar code medication administration technology: A systematic review of impact on patient safety when used with computerized prescriber order entry and automated dispensing devices. The Canadian Journal of Hospital Pharmacy, 69(5), 394-402.
