Polycystic ovary syndrome (PCOS) is a pathology of the system and functions of the ovaries. The crucial characteristic is ovarian hyperandrogenism with impaired menstrual and generative function. PCOS is a polysymptomatic disease accompanied by hyperandrogenism, menstrual dysfunction, impaired production of woman sex hormones, and cystic fluctuations in the ovaries, which are detected by ultrasound. Within the global scope, “women of reproductive age accounted for 1.55 million (95% uncertainty intervals (UIs): 1.19–2.08) incident cases of PCOS and 0.43 million (0.19–0.82) associated DALYs [associated disability-adjusted life-years] (Liu et al., 2021, p. 1108).
Throughout the recent period, the related shifts may be presented as follows. According to Liu et al. (2021), “The global age-standardized PCOS incidence rate among women of reproductive age increased to 82.44 (64.65–100.24) per 100 000 population in 2017, representing an increase of 1.45% (1.43–1.47%) from 2007 to 2017” (p. 1108). These numbers show the notable presence of the disease in the world, which justifies constant research in the area.
PCOS Essentials
Microscopic examination of the ovaries in the case of the disease shows a significant thickening of the tunica albuginea; its compaction and even hardening take place. The ovarian cortex is represented by primordial follicles. As a rule, primary follicles are usually unchanged, while secondary and tertiary follicles are exposed to pronounced cystic damage. Follicular cavities acquire the shape of a circle or oval, less often, a gap. On the walls of the follicles, folds appear, facing the inside of the enlarged follicle cavity (Rondanelli et al., 2020).
Granular cells undergo dystrophic changes and often desquamate into the lumen of the cavity. In some enlarged follicles, one or more layers of granulosa cells can be found lining the inner surface of the cystic cavities. These layers of granulosa cells do not have clear boundaries and turn into an overdeveloped, sharply hyperplastic outer follicle membrane.
With polycystic degeneration of the ovaries, a pronounced theca-cellular reaction is noted around most follicular cysts; theca cells are small, oval, or elongated. Their protoplasm is usually poorly stained, and small lipid inclusions are often found in it, the presence of which is associated with the supposed secretion of progesterone and its derivatives by these cells. There are also androgenic steroid hormones that cause the development of the female body according to the male type.
Several types of theca internal structure should be distinguished (Meier, 2018). The most common is the so-called insufficiently differentiated inner membrane of the follicle, accompanied by the proliferation of fibroblast-like cellular elements resembling cells of the outer membrane of the follicle. These cells surround the cystic follicle and pass into the outer membrane, which is then sharply hyperplastic. The second type is the inner lining of the follicles, which resembles that of intact or mature Graaf vesicles.
In the ovaries with signs of polycystic disease, there are generally no functionally active yellow bodies, but sometimes you can find small formations with indistinct contours and diffuse hemorrhage in the center. The cortical substance of the ovaries affected by polycystic disease contains a certain number of undeveloped primordial follicles, as well as atretic bodies (Witchel et al., 2019). There is pronounced hyperplasia of stromal cells, which, intensively developing, fill almost completely the medulla and penetrate into the elements of the cortical layer of these organs. The ovarian stroma is formed by spindle-shaped cells – fibroblasts, which are closely adjacent to each other and have no clear boundaries. In this regard, during a microscopic examination, the nuclei of these cells, which are elongated, are most often distinguishable.
Sometimes in the ovarian stroma, there are areas of more frequently located nuclei. These areas, apparently, arise as a result of focal cell hyperplasia. Figures of mitosis can often be found among such cells (Rondanelli et al., 2020). The cellular elements of the interstitial tissue can sometimes undergo luteinization. In some cases, pathological processes of the opposite nature are observed in the ovarian stroma. Among the cellular elements of an epithelioid nature, there are areas of growth of connective tissue, the number of cells decreases, and almost the entire stroma is sometimes subjected to such sclerosis, and sometimes only its individual areas.
Among the manifestations of PCOS are the following: menstrual irregularities, hirsutism, alopecia, hyperinsulinemia, disorders of carbohydrate and lipid metabolism, obesity, insulin resistance, mental disorders, and infertility. According to modern criteria, the presence of two of the three criteria in a patient simultaneously makes it possible to diagnose PCOS in the event that other pathological conditions are excluded. Modern international diagnostic criteria include the following features (Williams et al., 2016). First, there are signs of polycystic ovaries according to pelvic ultrasound; second, it is oligo- or anovulation; third, these are clinical or biochemical manifestations of ovarian hyperandrogenism. It should be noted that testing follicle-stimulating hormone (FSH) and luteinizing hormone (LH) ratio, given that normally, it is 1:1. “In women with polycystic ovaries, the LH to FSH ratio is often higher – for example, 2:1, or even 3:1” (Advanced Fertility Center of Chicago, n.d., para. 21).
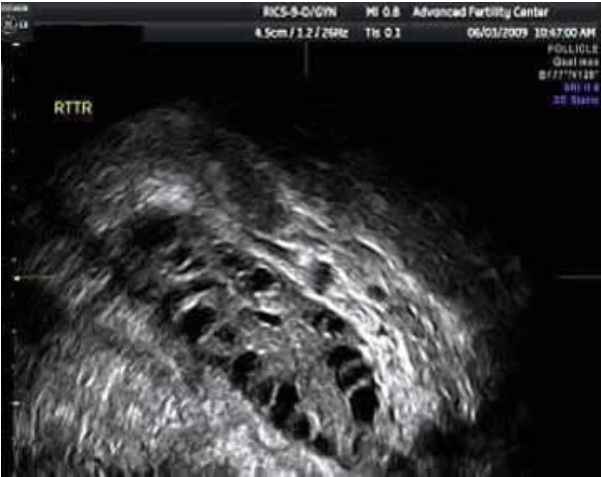
Ultrasound Images

Treatment
It is imposible to completely get rid of PCOS; however, there is the opportunity to support the body by taking medications. First of all, doctors prescribe medication, which involves hormonal drugs and their antagonists. The selection of such funds is carried out on a strictly individual basis since it will be necessary to replace the missing hormone and reduce the production of excessively present. Further, these are agents that cause a decrease in blood sugar levels (Mohammadi, 2019). It is advisable to take them because, in this way, it is possible to normalize the sensitivity of tissues to insulin and reduce its concentration in the blood. Vitamin complexes should also be noted – they are needed to maintain the immune system. B vitamins have significant effects on the functionality of the reproductive system.
Treatment of PCOS differs in duration – therapy should last at least six months. If, during the specified period, there are no positive dynamics of the disease, then the gynecologist can refer the patient to surgery (Escobar-Morreale, 2018).
However, often, it is conservative appointments that solve the problem. Conception often occurs – even multi follicular polycystic ovary disease and pregnancy are quite compatible. Among crucial medications, the following ones can be named: Clomiphene (50 to 100 mg/day), Metformin (1500 to 2250 mg/day), Rosiglitazone (2 to 8 mg/day) (Radosh, 2009). Spironolactone can be viewed as a notable alternative with 50 to 100 mg daily intake. However, it is not FDA approved, which justifies concerns regarding this option (Radosh, 2009). Drowsiness, weakness, and increased urination are common side effects that the mentioned drugs can cause.
Diet
With polycystic ovary disease, diet is an important point in the process of correcting a pathological condition. Therefore, the approach to drawing up the regime must be serious. The use of various forms of weight loss, which is based on a voluntary refusal of food, is unacceptable. Diet development is carried out by specialists in the field of dietetics. Each weight loss program is made individually, taking into account the woman’s life history. The polycystic ovarian diet is about bringing abnormal body weight to the normal range without further increasing it.
Frequent eating in small portions consists of 5-6 meals a day and helps to reduce the daily calorie intake by reducing the need for food. The number of calories consumed should correspond to energy consumption. The recommended calorie content is no more than 1800 kcal/day. Eating foods with a low glycemic index (less than 50, slow carbohydrates) is the main indicator of the effect of food on glucose levels in the body. Periodic use of products with an index of 51-70 is permissible. With polycystic disease, there is a risk of developing diabetes mellitus since the body is in a hormonal imbalance. The correct balance of carbohydrates, proteins, fats contributes to the proper functioning of the body. Eating fiber, in turn, detoxifies the body, lowering glucose and cholesterol levels.
Prognosis
With proper treatment and observation of females with polycystic ovary disease, a regular menstrual function is restored, hirsutism is compensated for, as well as weight loss occurs. Fertility recovery occurs in approximately 70% of females with the disease (Barber et al., 2016). With age, PCOS symptoms level off, and women in the older age group require contraception. If you do not contact a gynecologist about menstrual irregularities and possible polycystic ovary disease, then the possible long-term consequences. In females who have polycystic ovary, hypertension is much more common, and the risks of myocardial infarction, type 2 diabetes mellitus, and endometrial cancer are increased.
References
Advanced Fertility Center of Chicago. (n.d.). Polycystic ovarian syndrome (PCOS): Tests for PCOS – how to make the diagnosis? Web.
Barber, T. M., Dimitriadis, G. K., Andreou, A., & Franks, S. (2016). Polycystic ovary syndrome: insight into pathogenesis and a common association with insulin resistance. Clinical medicine (London, England), 16(3), 262–266.
Escobar-Morreale, H. F. (2018). Polycystic ovary syndrome: definition, aetiology, diagnosis and treatment. Nature reviews. Endocrinology, 14(5), 270–284.
Liu, J., Wu, Q., Hao, Y., Jiao, M., Wang, X., Jiang, S., & Han, L. (2021). Measuring the global disease burden of polycystic ovary syndrome in 194 countries: Global Burden of Disease Study 2017. Human Reproduction, 36(4), 1108–1119.
Meier R. K. (2018). Polycystic ovary syndrome. The Nursing clinics of North America, 53(3), 407–420.
Mohammadi M. (2019). Oxidative stress and polycystic ovary syndrome: A brief review. International journal of preventive medicine, 10, 86. Web.
Radosh, L. (2009). Drug treatments for polycystic ovary syndrome. American Family Physician, 79(8), 671–676.
Rondanelli, M., Infantino, V., Riva, A., Petrangolini, G., Faliva, M. A., Peroni, G., Naso, M., Nichetti, M., Spadaccini, D., Gasparri, C., & Perna, S. (2020). Polycystic ovary syndrome management: a review of the possible amazing role of berberine. Archives of gynecology and obstetrics, 301(1), 53–60.
Williams, T., Mortada, R., & Porter, S. (2016). Diagnosis and treatment of polycystic ovary syndrome. American Family Physician, 94(2), 106–113.
Witchel, S. F., Oberfield, S. E., & Peña, A. S. (2019). Polycystic ovary syndrome: Pathophysiology, presentation, and treatment with emphasis on adolescent girls. Journal of the Endocrine Society, 3(8), 1545–1573.
