Arterial hypertension is a condition of persistently raised blood pressure (BP), systolic BP more than 130 mm Hg, and diastolic more than 80 mm Hg. The origin of the essential, or primary, arterial hypertension is unknown. The condition is a major issue of up-to-date medicine as it causes several pathological conditions affecting various body systems and is frequently a silent killer. A significant part of individuals does not feel high blood pressure and does not take treatment. According to an AHA report by Casey et al. (2019), more than 100 million Americans have high BP, and 20% of US adults were unaware of having the condition. In this assignment, I will mostly focus on the high blood pressure’s interconnections with renal, pulmonary, and circulatory systems and compensatory mechanisms initiating in them.
The origin of the primary condition is unknown, nowadays we precise its development as a combination of genetic predisposition and environmental factors influence such as salt intake, obesity, dyslipidemia, fasting blood glucose, physical activity, smoking, and some others. Some of the factors are non-modified: sex and race, age, premature menopause, and family history with HBP. Despite the fact we still research the origin of high BP, the mechanisms leading to various disorders are studied well. Essential arterial hypertension has a complex pathophysiology that is presented in figure 1.
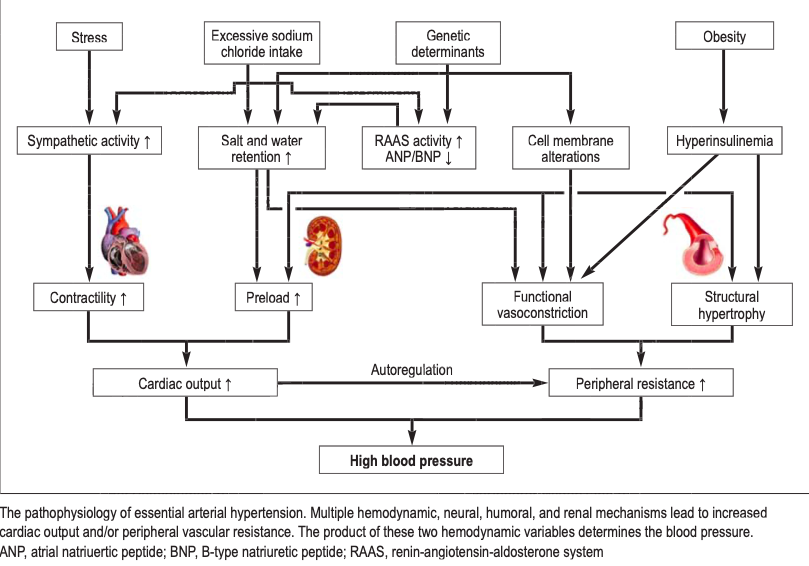
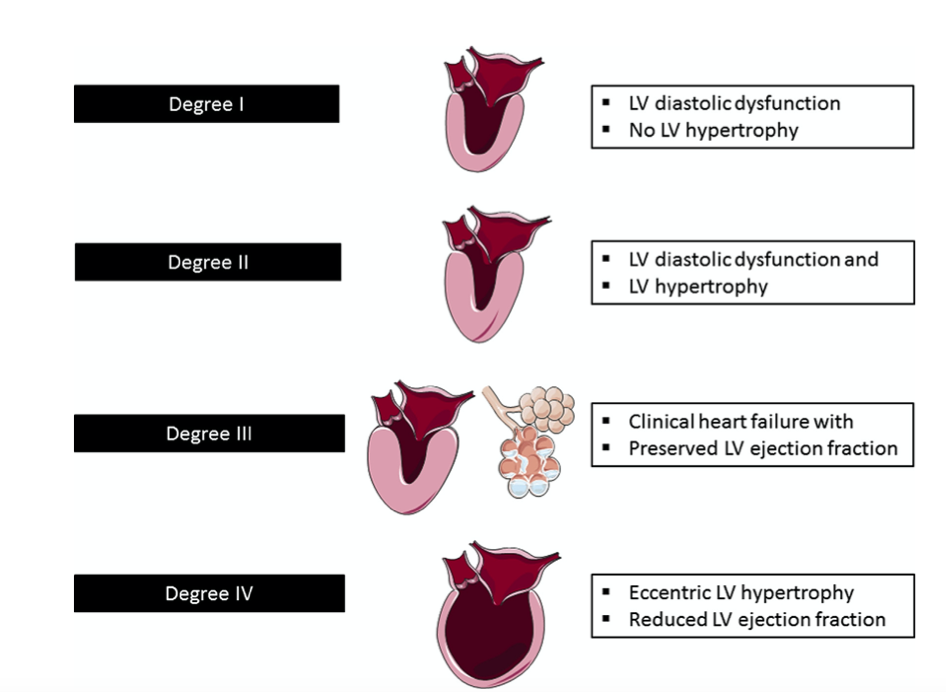
High blood pressure is an increased pressure pushing on vessel walls that damages them within time. With such numerous alterations, constant vessel constriction, high sympathetic activity heart muscle cells react by changing the structure increasing the muscle tissue size. This regulative mechanism is called structured hypertrophy. The highest pressure is in the left ventricular as it is the last chamber pushing blood out. HBP causes left ventricular hypertrophy, and within time, fibrotic changes lead to progressive diastolic dysfunction causing insufficiency of the left atrioventricular valve (Slivnick & Lampert, 2019).
Raised pressure in the right atrium dilatates the chamber and later causes pulmonary hypertension which leads to tachypnoea, lung fibrosis, and pulmonary edema in the late stages of the disease. Stages of hypertensive heart disease are shown in Figure 2.
The renal system’s activity relates to hypertension as kidneys filtrate metabolic products from the blood. Increased salt intake is associated with HBP, and commonly sodium, one of salt’s components was considered to increase plasma volume by attaching water molecules and, consequently, raising cardiac index and BP. Recent research claims that sodium directly affects vascular endothelium by constricting it (Garfinkle, 2017).
Also, when, during high salt loads, renal concentrating mechanisms reach maximum capacity, the body increases BP as autoregulation by rising total peripheral resistance of vessels (Garfinkle, 2017). The sensitivity of salt receptors reduces within years, respectively the risk of HBP grows parallelly with age.
Kidneys also take part in the renin-angiotensin-aldosterone system (RAAS) synthesizing renin in juxta-glomerular cells of renal glomerulus. Usually, when the intrarenal pressure is low, these cells take a signal to produce renin from its precursor, prorenin. Individuals with stable BP have a higher blood concentration of prorenin whilst humans with HBP have a prevalent renin synthesis (Saxena et al., 2018). With high pressure of liquids on vessel walls, the sympathetic activity raises which leads to vessel constriction and activation of beta-1 adrenergic receptors that induce renin production. Baroreceptors in afferent arteriole in kidneys also react on high BP and initiate renin synthesis: that is how RAAS starts working.
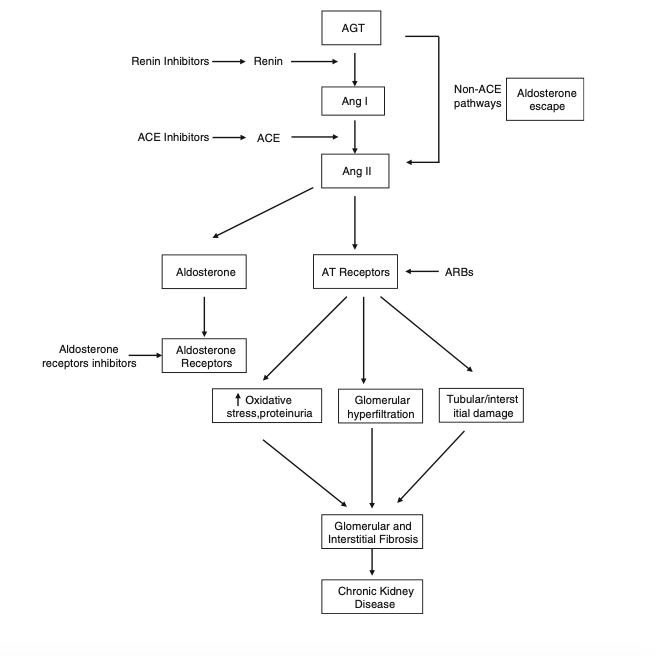
Renin hydrolyzes the other enzyme, angiotensinogen, to angiotensin I. Angiotensinogen is synthesized by the liver and the concentration of the enzyme in plasma can be elevated by estrogen, corticosteroid, and thyroid hormone (Patel et al., 2017). Peptide angiotensin I cleavages in lung capillaries, kidneys, and vessels to angiotensin II by angiotensin-converting enzyme (ACE). Angiotensin II constricts vessels, both arterials, and veins, and smooth muscles; stimulates the adrenal gland cortex to produce aldosterone. The last one influences sodium-potassium balance increasing sodium reabsorption and losing potassium with urine at the same time.
Angiotensin II also increases oxidative stress, proteinuria, lipogenesis, and intracellular calcium (Zhang et al., 2017). Hight pressure in renal vessels is chronic damage that leads to glomerular and interstitial fibrosis, a decrease of organ functioning. Angiotensin II is considered to be one of the major regulators of blood volume, pressure, and pH (Patel et al., 2017). Inhibitors of RAAS are widely used in the treatment of HBP and show high efficiency in a long-term perspective. RAAS elements are shown in Figure 3.
Hence, arterial hypertension is a condition creating multisystemic alteration and leading to various disorders of body systems. Increased pressure on vessel epithelium involves activity of RAAS, changes structural disorganization of heart muscle’s tissue, leads to insufficiency of the atrioventricular valve and a consequent HBP in lung vessels. To prevent further damages by HBP, people should insert into their routine measurements and screenings to correct the numbers of BP with target treatment in early stages.
Drug treatment of essential arterial hypertension is taken throughout all life; however, it prevents such co-morbidities as heart failure, pulmonary hypertension, retinopathy, and chronic kidney disease. Essential arterial hypertension remains one of the major issues in modern medicine. Averting modifiable risk factors and catching the condition in the beginning can put a positive impact on lifespan and quality of life.
References
Casey, D. E., Thomas, R. J., Bhalla, V., Commodore-Mensah, Y., Heidenreich, P. A., Kolte, D., Muntner, P., Smith S. C., Spertus, J. R., Windle, J. R., Wozniak, G. D., & Ziaeian, B. (2019). 2019 AHA/ACC clinical performance and quality measures for adults with high blood pressure: A report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. Circ Cardiovasc Qual Outcomes, 12(1), e000057. Web.
Garfinkle, M. A. (2017). Salt and essential hypertension: Pathophysiology and implications for treatment. Journal of the American Society of Hypertension, 11(6), 385–391. Web.
Jordan, J., Kurschat, C., & Reuter, H. (2018). Arterial hypertension. Diagnosis and treatment. Dtsch Artzebl International, 115(33-34), 557-568. Web.
Patel, S., Rauf, A., Khan, H., & Abu-Izneid, T. (2017). Renin-angiotensin-aldosterone (RAAS): The ubiquitous system for homeostasis and pathologies. Biomedicine & Pharmacotherapy, 94, 317–325. Web.
Saxena, T., Ali, A. O., & Saxena, M. (2018). Pathophysiology of essential hypertension: An update. Expert Review of Cardiovascular Therapy, 16(12), 879-887. Web.
Zhang, F., Liu, H., Liu, D., Liu, Y., Li, H., Tan, X., Liu, F., Peng, Y., & Zhang, H. (2017). Effects of RAAS inhibitors in patients with kidney disease. Current Hypertension Reports, 19(9), 1-7. Web.