Introduction
Background of Study
The provision of healthcare services has undergone several metamorphoses with patient quality and satisfaction being the core metrics for evaluating success. Patient satisfaction refers to the ability of healthcare workers to meet the expectations of their patients, as a key determinant of healthcare quality (Baek, Seo and Kim, 2016). Recently, there has been a push towards the adoption of patient-centered models in various health systems around the world (Zerwekh and Garneau, 2020). They encourage healthcare workers to treat patients with dignity and respect, as well as include them in decisions affecting their health and wellbeing (Baek, Seo and Kim, 2016). The push towards the adoption of patient-centered models of healthcare management has been a product of decades of searching for a framework that can integrate the interests of patients and healthcare service providers in healthcare service delivery (Baek, Seo and Kim, 2016). This process has been characterized by the interaction and variation of various interests in healthcare management to strike a balance between the provision of quality services and management of healthcare costs while promoting efficiency and improving patient satisfaction.
From this quest, many countries have accelerated the pace of adopting the patient-centered healthcare delivery model to accommodate the views of patients, family members, and healthcare service providers in developing healthcare plans (Adhikari et al., 2021). This has been made possible with the recognition of the importance of understanding and appreciating people’s diversity and individual interests when developing healthcare plans (Zerwekh and Garneau, 2020). The process has also encouraged healthcare professionals to recognize patients’ unique needs and interests by enabling them to understand the importance of respecting patients’ rights when making decisions on the kind of treatment plans suitable for them (Adhikari et al., 2021). Indeed, the focus on patient’s experiences emerges from a larger school of thought, which has been advanced by researchers, such as Baek, Seo and Kim (2016) that emphasize the importance of patients being treated with respect and dignity.
Overall, the patient-centered care model provides a framework for patients to ask questions about their care plans, give feedback on their medication experiences, and even compliment them if there is a need to do so. By doing so, patients feel more included and respected in the management of their health, thereby improving their satisfaction levels with services offered both within and outside the healthcare environment (Zerwekh and Garneau, 2020). Stemming from this development, the need to understand patient satisfaction is central in helping healthcare institutions to move towards adopting patient-centered models of healthcare management.
Problem Statement
People’s experiences when receiving healthcare services are an important determinant of their perceptions of service quality and satisfaction levels. However, it is difficult to accurately measure patient satisfaction standards, or their perceptions of healthcare quality, without understanding contextual factors limiting such experiences (Zerwekh and Garneau, 2020). For example, people’s experiences when receiving care are not only influenced by their opinions but also those of family and friends. Thus, it can be said that culture affects patient’s perceptions of quality and satisfaction. Additionally, the quality of healthcare services varies across countries and communities, thereby making it difficult to account for differences in patients’ backgrounds and cultures when evaluating their perceptions of quality and satisfaction. Therefore, it is important to understand the limitations that context-specific factors, such as culture and healthcare environment, have on our understanding of the relationship between patient satisfaction and service quality.
Research Gap
Patient satisfaction and quality healthcare services are integral to the adoption of the patient-centered models of healthcare management. This is especially true in the primary healthcare setting, which is the first point of contact between a patient and a healthcare service provider (Manzoor et al., 2019). A broad range of services is provided in this setting, including health promotion and prevention programs, which are essential to community growth and development, especially in low-income countries (Chi, Gutberg and Berta, 2020). The relationship between patient satisfaction and healthcare quality is rarely investigated in the primary healthcare setting even though most healthcare services are provided at this level (Chi, Gutberg and Berta, 2020). Furthermore, a majority of health professionals with private clinics, such as physiotherapy or dental practices, offer their services at this level of care delivery (Manzoor et al., 2019). Therefore, there is a need to understand the relationship between service quality and patient satisfaction in the primary healthcare setting because it is not only the first point of contact between patients and healthcare service providers but also a level of healthcare service delivery that encompasses a majority of healthcare services provided to patients.
Research Aim
To describe the nature of the relationship between quality healthcare services and patient satisfaction in the primary healthcare setting
Research Objectives
- To estimate the level of satisfaction patients have with the quality of services offered in the primary healthcare setting
- To determine the extent that socioeconomic variables affect the relationship between service quality and patient satisfaction in the primary healthcare setting
- To find out whether the relationship between patient satisfaction and service quality differs in primary and non-primary healthcare settings
Research Hypotheses
- H1. There is a positive relationship between healthcare service quality and patient satisfaction in the primary healthcare setting
- H2. Socioeconomic variables affect the relationship between quality healthcare services and patient satisfaction in the primary healthcare setting.
- H3. There are insignificant differences in the relationship between service quality and patient satisfaction in primary and non-primary healthcare settings
Significance of Study
Providing quality services to patients is one of the primary objectives of healthcare professionals. It is believed that when healthcare service providers do so, they improve patient satisfaction levels (Baek, Seo and Kim, 2016). Furthermore, some researchers have linked satisfaction with health services to positive health outcomes, such as high quality of life and enhanced levels of safety in the healthcare setting (Adhikari et al., 2021; Zerwekh and Garneau, 2020). Similarly, scholars have shown that satisfied patients are less likely to be admitted to emergency care units compared to unsatisfied patients (Zerwekh and Garneau, 2020). From an institutional perspective, some scholars have argued that improving satisfaction rates can lead to high patient retention rates, improved public image, and a diminished number of court cases (Baek, Seo and Kim, 2016). These statements suggest that having satisfied patients is good for the overall health of a community, institution, or country.
Stemming from the positive contributions of improved patient satisfaction levels on various stakeholders and indicators of healthcare quality, observers regard it as a critical measure of healthcare quality (Zerwekh and Garneau, 2020). The presents study aims to investigate the relationship between patient satisfaction and healthcare quality in the primary healthcare setting. Its findings will be useful to healthcare practitioners who want to gain a deep insight into key metrics of service quality that are relevant to improving patient satisfaction in the primary care setting. Improving patient satisfaction standards will have a direct positive effect on healthcare organizations and the communities they serve.
Structure of Paper
This paper is divided into five main sections. The first one is the introduction part, which provides a background to the study and sets the scene for undertaking the present study. Key items relating to the direction that the research will follow, including its aim, objectives, and hypotheses are explored in this section. The second chapter is the literature review section, which contains an analysis of what other scholars have written about the research topic. This review will lead to the third chapter of the paper, which is the methodology section. It describes strategies and techniques used by the researcher to test the hypotheses. Therefore, issues relating to design, approach, data collection, and analysis techniques will be discussed in this section of the paper. Thereafter, the findings of the analysis will be presented in the findings and discussion section, which is the fourth chapter of the study. The fifth and last section of the investigation is the conclusion and recommendations chapter, which provides a summary of the key findings and lists recommendations that would be adopted to improve patient satisfaction and quality of care in the primary healthcare setting.
Literature Review
Introduction
This chapter contains an analysis of what other researchers have said or written about the relationship between patient satisfaction and the quality of healthcare services. Therefore, it contains a review of extant literature that has discussed the relationship between healthcare quality and patient satisfaction. The aim of undertaking this analysis is to understand how the present study is positioned within the wider body of literature investigating the same research issue. To do so, factors affecting patient satisfaction and healthcare quality will be investigated to understand how they fit within different healthcare contexts.
Factors Affecting Patient Satisfaction
Understanding factors affecting patient satisfaction is central in improving the quality of healthcare services. This is because people have unique needs and preferences, which make it difficult for healthcare service providers to rely on one model of healthcare service provision to meet individual expectations. Furthermore, countries have different systems and models that affect the behaviors of their healthcare service providers and perceptions of satisfaction with healthcare services (Zerwekh and Garneau, 2020). These differences affect patient satisfaction levels because they moderate the behaviors of health professionals, influence the healthcare environment, and affect the social context through which the quality of health services are experienced.
Behaviors of Health Professionals
Healthcare professionals play a role in influencing the perceptions of patients towards the services they receive at a healthcare facility. Comparatively, the behaviors of health professionals are often influenced by an organization’s internal human resource strategies that are relevant to meeting patients’ needs and requirements (Manzoor et al., 2019). Therefore, the failure of human resource management could lead to low levels of patient satisfaction, while high levels of efficacy would lead to improved levels of patient satisfaction. The strength or weaknesses of a hospital’s human resource management strategies affect the behaviors of health professionals who are key players in the management of a healthcare institution’s value chain (Brower and Riba, 2017). In turn, patient satisfaction is affected by how the same professionals interact with patients.
The behaviors of health professionals have been classified in various forms but a majority of scholars use age differences to explain variations in attitudes that impact patient satisfaction (Zerwekh and Garneau, 2020). Particularly, they pay attention to four groups of health professionals: baby boomers (born between 1946-1964), veterans/traditionalists, who were born before 1946, Generation X, who were born between 1965 and 1947, and millennials who were born between 1980 and 1995 (Zerwekh and Garneau, 2020). Researchers say that when under stress, these groups of workers react differently, thereby leading to variations in patient outcomes. Broadly, these generational differences in the society that impact how health workers interact with their patients stem from differences in values and perceptions about healthcare management, which are primarily influenced by social norms and the peculiarities of the political and economic environment of the country or region.
Studies that have focused on the competence of health professionals in the delivery of quality services point to communication, empathy, and care coordination as critical skills that healthcare service providers need to have to improve their experience with patients (Adhikari et al., 2021). However, most health workers lack or are ill-equipped to use them (Manzoor et al., 2019). To remedy this problem, some researchers have proposed that hospital administrators should enhance their training programs to better equip healthcare workers with the skills needed to provide quality services (Brower and Riba, 2017). The main areas they can focus on include the improvement of interpersonal communications and relationship-building skills.
Healthcare Environment
The environment that hosts patients influences their care experience and their perceptions of the quality of services offered. In the present investigation, the hospital is the environment where care is given or provided to patients. It includes the hospital building and its surrounding physical spaces. Scholars have affirmed that the healthcare environment affects patient satisfaction (Chi, Gutberg and Berta, 2020). Although this relationship is positive, its formation is still unclear.
Discussions regarding factors affecting the healthcare environment have recently shifted towards understanding the impact that technology has on healthcare service provision. Particularly, researchers have taken a keen interest in understanding the role of the Internet of Things (IoT) in facilitating this shift (Baek, Seo and Kim, 2016). Stemming from this development, changes in the healthcare environment are seen to have an impact on patient satisfaction (Baek, Seo and Kim, 2016). Relative to this assertion, other researchers have explored the effect of the healthcare environment on patient satisfaction based on end-of-life care and established that poorly designed environments could frighten family members, especially those who visit their loved ones in intensive care unit (ICU) facilities (Sundberg et al., 2021). Therefore, the outlook of the hospital environment is crucial in improving the experiences of patients and family members when receiving care.
Stemming from this understanding, hospital administrators have been encouraged to rearrange furniture or refurbish patients’ rooms for improved comfort and ambiance (Sundberg et al., 2021). This statement affirms those of Chi, Gutberg and Berta (2020) which highlight the importance of maintaining a good ambiance in in-door and outdoor spaces for the healthcare environment while fusing it with a touch of nature because of its confirmed benefits to the healing process. Therefore, a supportive environment for healing is likely to positively influence perceptions of patient satisfaction (Sundberg et al., 2021). In this regard, the healthcare environment is a determining factor for patients’ satisfaction.
Socio-demographic Variables
The social setting and individual characteristics of a patient play a critical role in influencing patient satisfaction levels. Indeed, socio-demographic factors, such as age, gender, education qualifications, and income have been known to influence patient satisfaction (Taylor et al., 2021). Most investigations that have used demographic variables to explain health outcomes suggest that people with high-income and advanced education levels report better health outcomes compared to their counterparts who do not share similar characteristics (Gor et al., 2019). These findings have been developed after studying the health of different groups of respondents based on how they consumed illicit substances such as cigarettes and alcohol. It was established that the lack of education worsened their health outcomes and caused them to have low levels of satisfaction with their overall experiences (Bhattacharjee and Joshi, 2020). Therefore, these socioeconomic indicators can affect how patients rate their overall medical experience.
Generational differences among patients also affect their levels of satisfaction with healthcare quality. For example, Brower and Riba (2017) say that older patients prefer to be directed by their physicians regarding what they need to do to improve their health and wellbeing, while millennial patients want to work with their physicians in developing their care plans (Zerwekh and Garneau, 2020). These different views are likely to affect their perceptions of quality and satisfaction, including influencing how they view the work ethics of health professionals and their interpretation of a good healthcare environment. These same factors are likely to influence their relationship with authority, thereby affecting how patients interact with caregivers, who are also figures of authority in the healthcare setting. Their commitment to treatment plans and work ethic are also affected in the same manner.
Factors Affecting Healthcare Quality
Quality assurance is a critical part of healthcare service delivery and an essential component of quality improvement programs (Sundberg et al., 2021). The importance of maintaining high standards of quality in the healthcare setting has been highlighted in many pieces of literature, including those of Sundberg et al. (2021) and Adhikari et al. (2021). This section of the review shows that perceptions of quality are affected by a country’s model of health financing and differences in institutional practices.
Model of Health Financing
The resources available to a country or institution often influence healthcare service quality. Therefore, there is a need to understand how financing models impact service quality. Indeed, it is important to highlight these differences because they can affect how care is delivered or given to patients in various health facilities (Brower and Riba, 2017; Manzoor et al., 2019). Individuals who often run their healthcare facilities as businesses fund them privately but publicly funded medical facilities are run as state organizations that are not designed to maximize profit, but, rather promote the public good. The public vs. private structure model of financing has an impact on the kind of services a healthcare facility will offer because private institutions often require patients to pay higher costs to access quality services, while public healthcare facilities do not have such stipulations because of their aim, which is not to maximize profit. However, these facilities also have their challenges, which may undermine service delivery. For example, Manzoor et al. (2019) say, “in public sector hospitals, there are numerous patients, heavy workloads for staff, and a work environment where physicians/doctors can behave rudely” (p. 3318). Therefore, there is a difference in the quality of care offered in public and private healthcare facilities.
Institutional Differences and Workplace Practices
Institutional differences in workplace attitudes towards the provision of healthcare services have also influenced the quality of care offered at different healthcare facilities. This difference in outcome is rooted in variations in work ethic across different groups of health workers based on their organizational cultures. For example, a book by Brower and Riba (2017) suggests that institutional differences can be best solved by embracing practices that promote diversity and productivity at the same time. For example, a new generation of professionals can introduce their older counterparts to a different way of completing tasks, thereby leading to new levels of task orientation.
Summary
The evidence adduced in this paper shows that the relationship between patient satisfaction and quality of healthcare services has been mostly investigated from the non-primary care setting. However, the present study aims to investigate the same relationship from the perspective of the primary care setting. Consequently, it is important to have a contextualized understanding of the relationship between patient satisfaction and quality of healthcare to fill the emerging research gap. It is defined by the lack of insight into how the same relationship plays out in non-western countries and those that do not have the same healthcare models as those applied in western nations.
Methodology
Introduction
This chapter describes techniques used by the researcher to answer the study questions. The items explored in this section of the review stem from the framework provided by Melnikovas (2018) in explaining the methodology of a study. He suggests that research studies are conducted in five spheres, including philosophy, approach, strategies, choices, and time horizons, as described in figure 3.1 below.
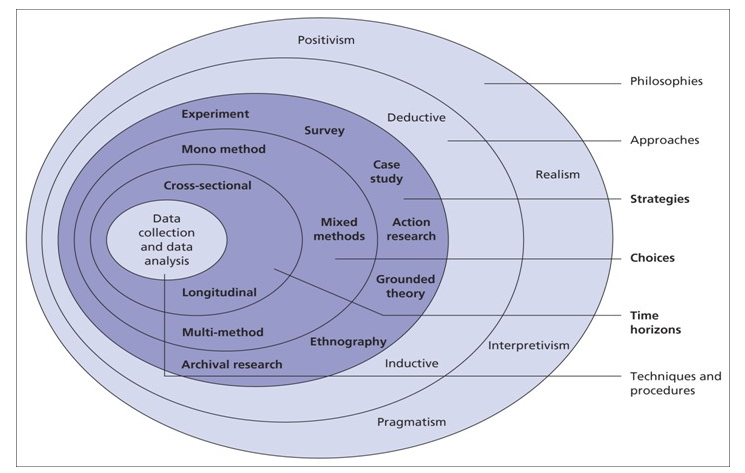
The researcher used the items described above to inform the format of this chapter as outlined below.
Research Philosophy
It is important to review the philosophy used in a study to understand a researcher’s belief in the way data was collected, disseminated, and analyzed. There are four main philosophies in research: interpretivism, positivism, pragmatism, and realism (Melnikovas, 2018). The positivism research philosophy is grounded in the belief that the world can be explained objectively by focusing on a problem. This research philosophy implies that practical results are instrumental in answering research questions. Comparatively, the realism research philosophy suggests that reality can be independent of the human mind (Melnikovas, 2018). Therefore, it emphasizes the need to view the world through personal lenses. The pragmatism research philosophy encourages researchers to select techniques that would best answer their research problems (Melnikovas, 2018). Alternatively, the interpretivism research philosophy evaluates the role of the researcher in evaluating the social world (Melnikovas, 2018). Based on the nature of the above-mentioned research approaches, the interpretivism research approach emerged as the best fit for the present investigation. Its selection is informed by the subjective nature quality and satisfaction elements of healthcare service delivery. Therefore, it is important to analyze the two variables from the actors at play.
Research Approach
Two main research approaches are used in academic studies – inductive and deductive reasoning. The deductive technique works by using broad generalizations of research issues to create one coherent narrative. Comparatively, the inductive research approach uses one narrative to generalize about a specific research issue. Given that the present study evaluated the relationship between quality healthcare and patient satisfaction, by focusing on one region in Saudi Arabia, the inductive research approach emerged as the best fit to use in the investigation. It facilitated the use of findings generated from one region of Saudi Arabia to make generalizations about the effects of healthcare quality on patient satisfaction.
Research Strategy
As highlighted in figure 3.1 above, researchers can use seven strategies in academic investigations and they include surveys, experiments, case studies, action research, grounded theory, ethnography, and archival research. The case study approach was used in the current investigation because evidence of the relationship between healthcare quality and patient satisfaction was derived from one case, which is at a primary healthcare facility in the Eastern region of Saudi Arabia.
Research Choice
The quantitative research approach was used as the main research choice for the present investigation. It is primarily preoccupied with the use of statistical methods to answer a research question. In other words, the researcher quantified the relationship between healthcare services and patient satisfaction by generating numerical data using surveys to create a set of numerical variables that were later assessed and analyzed to address the research issue. The quantitative research choice was also adopted because it was the most appropriate technique to use in testing the research hypotheses.
Time Horizon
Research variables can be assessed using either cross-sectional or longitudinal methods. Cross-sectional research is often used in situations where variables are assessed over a specific period. Alternatively, the longitudinal research technique is applied when research intends to measure variables over a long time. Based on these differences, the cross-sectional time horizon was used for the present study because it is descriptive. The longitudinal research method was not used in the study because the researcher did not intend to measure the causality of variables, but rather describe them. Therefore, the cross-section time horizon method emerged as the most suitable technique to use in the study.
Research Instruments
The researcher collected data from a structured survey, which was adapted from the Hospital Consumer Assessment of Healthcare Providers and Systems Survey (HCAHPS), which was developed by the Massachusetts Medical Society (2018). This data collection tool was selected for use in the present study because it has been widely used in the healthcare field to measure patient satisfaction based on the quality of healthcare services offered. Indeed, the survey instrument was developed by two reputable healthcare agencies – the Centers for Medicare and Medicaid Services (CMS) and the Agency for Healthcare Research and Quality (AHRQ) (Massachusetts Medical Society, 2018). The data collection instrument was also selected for use in the study because it standardizes patients’ experiences into measurable formats that can be used to assess healthcare quality across different hospitals.
The surveys were in two parts: the first one was instrumental in collecting demographic data relating to the respondents, where three variables, identified as A1, A2, and A3, representing the respondents’ age, gender, and education qualifications, were used to obtain demographic data. These variables were included in the study because they have been proved to affect patients’ perceptions of healthcare quality and satisfaction standards (Adhikari et al., 2021; Massachusetts Medical Society, 2018). Other questions posed to the respondents were aimed at assessing the relationship between healthcare service providers and their patients by analyzing the outcome of their encounter using six key criteria of performance: nursing care, hospital environment, doctor’s care, hospital experiences, pharmacy experiences, and overall hospital rating. Collectively, these measures of patient satisfaction and perceptions of the quality of services offered at the healthcare facility have 19 items of measurement. All of them were substantive items that described patients’ critical care experiences based on the criteria outlined by the Massachusetts Medical Society (2018) describing the relationship between patients’ satisfaction levels and the care of healthcare services provided in hospitals. They include communication with doctors, state of cleanliness in the hospital environment, the serenity of the healthcare setting, hospital experiences, pharmacy experience, and a hospital’s overall rating (see appendix 1).
The above-mentioned areas of communication helped the researcher to assess a patient’s overall satisfaction levels with the quality of services offered at the healthcare facility. The researcher measured the intensity of their responses in five key levels: “strongly agree,” “agree,” “neither agree nor disagree,” “disagree,” and “strongly disagree.” It is believed that this 5-point Likert scale has high scale sensitivity, which was instrumental in helping to understand the intensity of the respondents’ views. It has also been used to measure the views of patients in several healthcare settings (Massachusetts Medical Society, 2018). Therefore, the justification for its use in the current research setup stemmed from its wide applicability in the healthcare field; particularly, in measuring patient satisfaction.
Research Participants and Sampling Method
Informants were patients who had received primary healthcare services at a hospital facility in the Eastern Region of Saudi Arabia. The researcher identified participants by the kind of services they received at the hospital facility. As highlighted in chapter 1 of this paper, the focus of the investigation was on describing the relationship between the quality of services offered in the primary healthcare setting and the contentment of patients with the care offered. Therefore, to gain access to patients who had received such kinds of services, the researcher only contacted patients who had met a dentist, counselor, dietitian, osteopath, or physiotherapist, as the main primary healthcare services offered at the medical facility.
Based on the above identifying criteria, the researcher recruited 60 health professionals working at a public health facility in the Eastern region of Saudi Arabia. The researcher invited the respondents to take part in the study by filling a structured questionnaire administered online. The informants were recruited using the purposeful sampling method. It works by allowing a researcher to gain access to participants through referrals (Massachusetts Medical Society, 2018). One informant was an acquaintance of the researcher who later introduced them to others who were willing to take part in the investigation. The purposeful sampling method was selected because the researcher wanted to sample the views of health workers who were knowledgeable about patient satisfaction and healthcare quality standards in their workplace.
Data Analysis
The researcher completed the data analysis using the Statistical Packages for the Social Sciences (SPSS) software, which employs various descriptive and inferential data analysis techniques to analyze information (Melnikovas, 2018). This data analysis method has been hailed by different groups of users for the convenience it offers statisticians in managing complex data (Melnikovas, 2018). The researcher used descriptive and inferential analysis methods to decipher data using this software. It helped to explain the meaning of the data using concise computational techniques.
Research Ethics
Other ethical considerations in the study were consent, treatment of data, and confidentiality of data. These issues are discussed below.
Consent: One of the foundational principles of research ethics is obtaining informed consent from researchers who freely choose to take part in a research investigation with full knowledge of what it entails (Melnikovas, 2018). In line with these guidelines, respondents who took part in the investigation did so voluntarily. Stated differently, the researcher did not coerce them or provide financial incentives for the respondents to take part in the study. The aim of doing so was to maintain objectivity in the research by obtaining views from people who wish to give their honest views on the subject matter. Therefore, the researcher only sought the views of respondents who gave their consent freely to take part in the investigation.
Anonymity and Confidentiality: The views of the respondents were presented anonymously to protect their identity from any consequences that may arise out of participating in the study. Therefore, no identifiable variable relating to the informant’s names was included in the study. This strategy is consistent with the views of Melnikovas (2018), which encourages researchers to take necessary steps to ensure the protection of private data. The confidentiality of the respondents was also guaranteed in the course of developing this research by taking necessary steps to make sure others do not discover the identity of the respondents. The data analysis process helped to achieve this objective by delinking the respondent’s views from their names using codes that were presented in the SPSS codebook. Therefore, the researcher only presented aggregate data as opposed to individual-level analysis
Treatment of Data: The information obtained by the respondents was stored safely in a computer and secured using a password. This measure was taken to minimize the possibility of unauthorized persons accessing the data and altering it or taking information without consent. The different measures taken to safeguard the ethical implications of this study were aimed at protecting the interests of the respondents at different stages of the research, including collection, dissemination, and analysis of data. After the research process is completed and the purpose of the investigation fulfilled, the researcher will destroy the information to further prevent unauthorized use for any other purpose besides what was originally intended. The measures taken to protect the integrity of data are consistent with the views of Melnikovas (2018), which also emphasizes the importance of researchers to take necessary measures to protect the integrity of information collected from respondents. As the last step in the ethical review process, the researcher made sure that the above-mentioned processes did not contravene ethical rules and principles outlined by the Swiss Business School (SBS). The aim of doing so was to make sure that all the steps taken were consistent with the institution’s guidelines on writing theses and dissertations.
Limitations of Study
The findings highlighted above are limited to the primary healthcare setting. This means that they are mostly relevant to patient satisfaction standards when they seek medical services as the first point of contact with a health system. This limitation stems from the nature of the primary healthcare setting, which is designed to offer medical services in this manner. This analysis means that most of the information presented in the document is relevant to the primary healthcare setting, which represents most healthcare care services provided in the community health centers. The findings of this study could be extrapolated to healthcare professionals who offer auxiliary primary health services, such as dentists and gynecologists.
Findings and Discussion
Introduction
The section of the study relates to the findings obtained from applying the above-mentioned methodology. For the descriptive analysis part of the analysis, information relating to the respondents’ gender, age, and education qualification were quantified to understand their influence on perceptions of healthcare quality and patient satisfaction.
Demographic Findings
The demographic characteristics of the respondents were quantified according to their gender, age, and education qualifications as highlighted above. The findings are depicted below.
Gender
The first demographic variable analyzed in this study was gender. This was a dichotomous variable with two codes, denoted by numbers 1 and 2, to represent male and female respondents. According to table 4.1 below, 60 participants took part in the study with a majority of them being male (36 people), while females were 24.
Table 4.1 Classification of respondents according to gender
Education Qualification
The effects of education on health outcomes have been documented in several studies that have analyzed its impact on health outcomes (Gor et al., 2019; Baek, Seo and Kim, 2016). This is the justification for including this variable in the study. The respondents were required to state their highest education qualifications with the lowest education qualification being 8th grade and the highest being a Ph.D. The findings of the review are highlighted in table 4.2 below.
Table 4.2 Classification of respondents according to education qualifications
As highlighted in figure 4.2 above, most of the respondents (50%) had a high school education certificate, while the second-largest group of participants (20%) had a diploma. The smallest group of informants had a bachelor’s degree and they represented 3.3% of the total sample.
Age
Age was the fourth demographic variable investigated in the study. This variable was included in the investigation because of the effects of age on the work ethics of healthcare professionals and their impact on patient’s perceptions of quality and satisfaction with healthcare services. The respondents had five options to choose from with the lowest age group comprising of people between 18 and 25 years, while the oldest demographic was made up of people who were older than 55 years. The respondents were classified along these lines as outlined in table 4.3 below.
Table 4.3 Classification of respondents according to age
According to the findings highlighted above, most of the respondents who took part in the investigation were above 55 years old, followed by those who were between 46 and 55 years. This could be because older people are more prone to illnesses compared to younger people. Therefore, they are likely to seek primary healthcare services more than any other demographic.
Descriptive Statistics
This second part of the data analysis process was instrumental in understanding the respondents’ views on the different aspects of care offered to them at the facility. To determine their responses, the descriptive analysis technique was used to assess their mean, standards of deviation, and variances as highlighted in table 4.4 below.
Table 4.4 Descriptive statistics
As highlighted in table 4.4 above, most of the respondents had a favorable or neutral view of the statements posed to them. This is because the means for the items sampled oscillated between 1 and 3 signifying a favorable response. Stated differently, most of the participants agreed with the statements posed, implying that they were generally satisfied with the service offered at the facility. However, there were significant gaps in communication between the healthcare staff and the respondents when it came to discharging patients and explaining the purpose of the medications. This is because this area of research attracted responses with a mean of 3, signifying the lack of agreement or disagreement with the questions posed. In this regard, there is a gap in service delivery that needs to be improved through improved relationships between patients and healthcare staff.
Impact of Demographic Variables on Findings
It was necessary to understand the impact of demographic variables in the study because it was the third research objective, which sought to understand whether socioeconomic variables impacted patient’s views of healthcare quality and satisfaction levels. Furthermore, it was necessary to undertake a demographic review of the findings because data highlighted in table 4.6 above were not controlled for age, gender, and education levels. The impact of these variables on the findings is explained below.
Age
The impact of the respondents’ age on the findings was assessed using the one-way ANOVA method and the findings are depicted in table 4.5 below.
Table 4.5: Impact of age on findings
According to the findings highlighted in table 4.5 above, age did not have a significant impact on the findings because most of the questionnaire items had a significance value below p>0.05. This means that the views of the respondents were not influenced by their ages. This could be because of the largely homogenous nature of the Saudi population.
Gender
The impact of the respondents’ gender on the findings was also assessed using the one-way ANOVA method and the findings are depicted in table 4.6 below.
Table 4.6: Impact of age on findings
According to the findings highlighted in table 4.6 above, gender had an insignificant impact on the findings because most of the questionnaire items had a significance value above p>0.05. This means that the views of the respondents were not influenced by their ages.
Education Level
The impact of the respondents’ education levels on the findings was also assessed using the one-way ANOVA method and the findings are depicted in table 4.7 below.
Table 4.7: Impact of education levels on findings
The findings highlighted in table 4.7 above show that only two items had a significance value below p<0.05. This means that education levels did not affect the views of the respondents. Collectively, the findings of this demographic analysis suggest that none of the demographic variables significantly affected the views of the respondents towards patient satisfaction. This finding means that the findings of this investigation are inconsistent with those that have demonstrated the effects of age, education level, and gender on patients’ satisfaction levels. Again, this disparity in findings can be explained by the homogenous nature of Saudi society.
Summary
The findings of the study showed a positive relationship between the quality of health and patient satisfaction in the primary care setting, signifying the acceptance of the first hypothesis (H1), which affirmed the same position. Comparatively, H2 is rejected because the demographic variables did not impact the findings. Comparatively, H3 was accepted because there were insignificant differences in the relationship between healthcare quality and patient satisfaction in primary and non-primary care settings.
Conclusion and Recommendations
Conclusion
From the onset of this study, the researcher strived to understand the relationship between service quality and the extent that patients are satisfied with services received in the primary healthcare setting. Three research objectives guided this investigation. The first one was designed to investigate the relationship between the quality of services offered at primary healthcare facilities and the level of contentment with the same services. The second one is set to determine the extent that socioeconomic variables affect the relationship between quality healthcare services and patient satisfaction in the primary healthcare setting. The last one was intended to find out whether patient satisfaction varied with the type of services offered at healthcare facilities.
The study was domiciled in Saudi Arabia, using a publicly funded healthcare organization in the Eastern region, as the setting for the study. The findings of the research showed a positive relationship between the quality of health and patient satisfaction in the primary care setting. H3 was affirmed because the findings showed that patient satisfaction does not vary with the type of services offered at healthcare facilities. This statement suggests that the relationship between service quality and satisfaction is consistent in both primary and non-primary healthcare settings. Therefore, healthcare service providers may adopt similar behaviors and traits in different healthcare settings.
H1 was also affirmed because there was a positive relationship between service quality and patient satisfaction, meaning that the quality of healthcare services offered significantly affected the degree of patient satisfaction. Comparatively, H2 was rejected because the relationship between service quality and contentment with healthcare services did not vary across populations of people with different backgrounds or socioeconomic profiles. This finding is inconsistent with others described in the literature review section of this paper, which suggested that demographic variables affected patient satisfaction levels. The inconsistency could be because of the homogenous nature of the Saudi society, especially among patients who seek healthcare services in the Eastern region of the country.
Recommendations
The recommendations outlined in this section of the paper stem from the findings generated in this study, which show significant gaps in healthcare service provision from the perspective of healthcare staff management and the improvement of the environment that patients receive care. From these areas of governance and management, three recommendations are outlined below to improve patient satisfaction levels in the primary healthcare environment.
Improve Relationship between Patients and Healthcare Service Providers
The need to improve the relationship between patients and healthcare service providers comes from the low satisfaction index reported among patients for the care they received from doctors and nurses. The findings suggested the quality of care offered to patients in the primary care setting could be enhanced. Particularly, they highlight the importance of improving the relationship between patients and nurses because the latter are the primary caregivers in the primary healthcare setting. This statement draws attention to the importance of nurturing interpersonal skills especially among nurses and doctors who are the main health professionals active in the primary healthcare setting. Its importance in healthcare management has been highlighted by researchers such as Baek, Seo and Kim (2016) who categorize it as part of the people aspect of patient satisfaction.
The importance of improving interpersonal skills among healthcare workers in the primary care setting is further supported by the works of researchers such as Sundberg et al. (2021) and Adhikari et al. (2021) who highlight the importance of healthcare service providers to be empathetic and communicate well with their patients. For example, hospital staff may be encouraged to make rounds in patients’ rooms and ask if they are okay or if they need any help. Adopting such a strategy effectively requires hospital staff to have an open mindset where the needs and comfort of their patients are core priorities. Asking whether patients need assistance, or whether the temperature in their room is as desired, makes them have a good impression of the services received.
Adopting such proposals may require health administrators to train the nurses in providing more effective and up-to-date care practices. For example, healthcare service providers need to learn more about providing care to a diverse group of patients. Doing so will enable them to manage varying tastes, preferences, and expectations for care among different groups of people. This plan will also align with the recommendations of researchers such as Sundberg et al. (2021) and Adhikari et al. (2021), who highlight the importance of training healthcare staff to provide high-quality healthcare services in a diverse setting. Therefore, improving the relationship between patients and healthcare workers should be the priority for health administrators as it provides the foundation for the implementation of the other two recommendations listed below.
Align Hospital Policies with Quality Service Provision
An organization’s internal policies on healthcare quality management are instrumental in providing optimal support to patients who need such services. This statement stems from the role that hospital leadership and management play in ensuring high standards of quality are maintained in the healthcare setting. Their involvement also spans organizational processes and systems that support healthcare workers in providing high-quality care, such as purchasing equipment and tools that professionals need to provide services or making sure that the built environment is well maintained to the patient’s satisfaction.
Aligning a hospital’s policies and resources to institutionalize high-quality care would be instrumental in improving patient satisfaction. Doing so will make sure that the healthcare system prioritizes quality as a function of its overall health. These policy changes would address gaps and dysfunctional relationships between healthcare service providers by aligning policies, with organizations, methods, and capacities to provide optimum healthcare services to patients. The findings can further help to promote quality improvement processes in the non-primary care setting by drawing lessons from the primary care environment, which has been the focus of attention for the present study.
Improve Environment in Which Patients Receive Care
The importance of improving the environment where patients receive care is instrumental in boosting patient satisfaction levels because patients’ experiences are often enhanced via the healthcare environment. This recommendation draws its strength from the application of the place theory in the healthcare sector, which focuses on adopting a holistic view in the provision of high-quality care services. Overall, the recommendations outlined in this paper propose the use of a three-pronged strategy in improving patient satisfaction in the primary care setting by enhancing the relationship between patients and healthcare service providers, improving policy and procedures for managing quality issues in the healthcare environment, and improving the hospital environment for purposes of making a patients’ stay pleasant. These recommendations are intended to not only meet the needs of patients but also those of their friends and family who come to visit. It is part of a wider approach to healthcare management, which fuels the push towards a patient-centered healthcare management model.
Reference List
Adhikari, M., et al. (2021) ‘Patient satisfaction and its socio-demographic correlates in a tertiary public hospital in Nepal: a cross-sectional study’, BMC Health Services Research, 21(2), pp. 135-140.
Baek, S., Seo, S. H. and Kim, S. (2016) ‘Preserving patient’s anonymity for mobile healthcare system in IoT environment’, International Journal of Distributed Sensor Networks, 7(1), pp. 1-11.
Bhattacharjee, A. and Joshi, R. (2020) ‘Can your neighbour’s education affect your health?’, Journal of Health Management, 22(1), pp. 96–102.
Brower, K. J. and Riba, M. B. (2017) Physician mental health and well-being: research and practice. New York, NY: Springer.
Chi, P., Gutberg, J. and Berta, W. (2020) ‘The conceptualization of the natural environment in healthcare facilities: a scoping review’, Health Environments Research and Design Journal, 13(1), pp. 30–47.
Gor, B. et al. (2019) ‘Is socioeconomic advantage associated with positive health behaviors and health outcomes among Asian Indians?’, Health Services Research and Managerial Epidemiology, 3(1), pp. 1-11.
Manzoor, F. et al. (2019). Patient satisfaction with health care services; an application of physician’s behavior as a moderator. International Journal of Environmental Research and Public Health, 16(18), p. 3318.
Massachusetts Medical Society. (2018) Patient satisfaction surveys. Web.
Melnikovas, A. (2018) ‘Towards an explicit research methodology: adapting research onion model for futures studies’, Journal of Futures Studies, 23(2), pp. 29-44.
Sundberg, F. et al. (2021) ‘Visitor’s experiences of an evidence-based designed healthcare environment in an intensive care unit’, Health Environments Research and Design Journal, 14(2), pp. 178–191.
Taylor, J. et al. (2021) ‘Pediatric health outcome evaluation in low-and middle-income countries: a scoping review of NGO practice’, Global Pediatric Health, 6(2), pp. 1-10.
Zerwekh, J. and Garneau, A. (2020) Nursing today – e-book: transition and trends. 10th edn. London: Elsevier Health Sciences.