Abstract
The notion of burnout has long been an integral part of the preventive health care agenda. Over the past decades, various studies have demonstrated the relevance and benefits of burnout prevention. In a systematic review by Kleinpell et al. (2020), the issue of burnout is assessed both from the perspective of theoretical frameworks and empirical evidence gathered through a follow-up survey. The objective of the research was to assess the results of the burnout prevention summit in the ICU with the help of analyzing e-main survey responses. The lack of resources other than the ones presented by the CCSS creates a significant bias risk for the study. The results of the study demonstrate the summit’s relevance in the ICU context and justify the demand for burnout prevention. The CCSC’s explicit support, along with the lack of critical appraisal of the data, however, undermine the significance of the analysis.
Introduction
The issue of burnout has always been of critical importance in the context of health care, as fatigue and emotional distress inevitably result in higher exposure to medical errors and negative patient outcomes. The issue, however, is especially relevant to the intensive care units throughout the country, as the workload in such environments remains unprecedently high. For this reason, Kleinpell et al. (2020) decided to collect and analyze the professionals’ perception of burnout from the data presented at the National Summit and Survey on Prevention and Management of Burnout in the ICU.
According to the researchers, the core objective of this systematic review was “to summarize the results of expert discussions and recommendations from a National Summit and survey on promoting wellness and preventing and managing burnout in the ICU” (Kleinpell et al., 2020, p. 249). Hence, this systematic review placed major emphasis on analyzing the extent to which such organizations as the CCSC contributed to the promotion of anti-burnout interventions.
Methodology
There was no extensive protocol for the studies selection, as the only data eligible for the systematic review included the expert opinions presented during the summit in the question and the follow-up burnout syndrome survey. The survey was sent to the participants via an e-mail database. Thus, the eligibility criteria for the analysis were rather limited and included exclusively the studies and questionnaires correlated to the CCSC summit and call to action (Kleinpell et al., 2020). However, as far as the survey eligibility criteria are concerned, the primary exclusion criterion of the research was the absence of the CCSC membership and access to the summit materials. The information sources for the study include the following primary documents:
- Critical Care Societies Collaborative (CCSC) Statement on Burnout Syndrome in Critical Care Healthcare Professionals: A Call for Action;
- CCSC’s National Summit on Prevention and Management of Burnout in the ICU;
- a descriptive survey on strategies for addressing burnout using Research Electronic Data Capture (REDCap) (Kleinpell et al., 2020, p. 249).
No search strategies like keywords and Boolean logic were employed during the analysis, as the three major documents were pre-selected, and the supplemental data were extracted from the documents described above. The selection of the studies was based on the principle of correlation to the CCSC summit in question, whether it was summit expert statements or studies used in the “Call to Action” (Moss et al., 2016).
The data collection patterns had two major approaches: document and record collection and a survey. The former was used to analyze the information presented in both the pre-summit research paper and the summit per se. During the pre-summit research, the underlying variables of the research included anti-burnout interventions, including organizational and individual measures as an independent variable, and burnout syndrome rates as a dependent variable. Later, the same variables, along with the burnout awareness, were analyzed with the help of a follow-up survey.
The exclusion of any other studies unrelated to the CCSC activity presents a bias for every study used in the research. Considering the fact that the initiation of the summit was encouraged by the findings outlined in Moss et al.’s (2016) review, it is necessary to define the existing biases in the study utilized. Out of approximately seventy sources used in the work, no references to state opposite points of view were presented, making the article lack an overall critical appraisal of the issue. The samples used in the studies were sufficient to draw tangible conclusions, but some samples studies were presented more than five years prior to Moss et al.’s (2016) research publication. The same bias of one-sidedness may be as well applied to the summit materials.
The summary measures included the survey population and the mean indicators of prevalent intervention techniques. Thus, the quantitative summary of the survey was introduced in the form of a table:
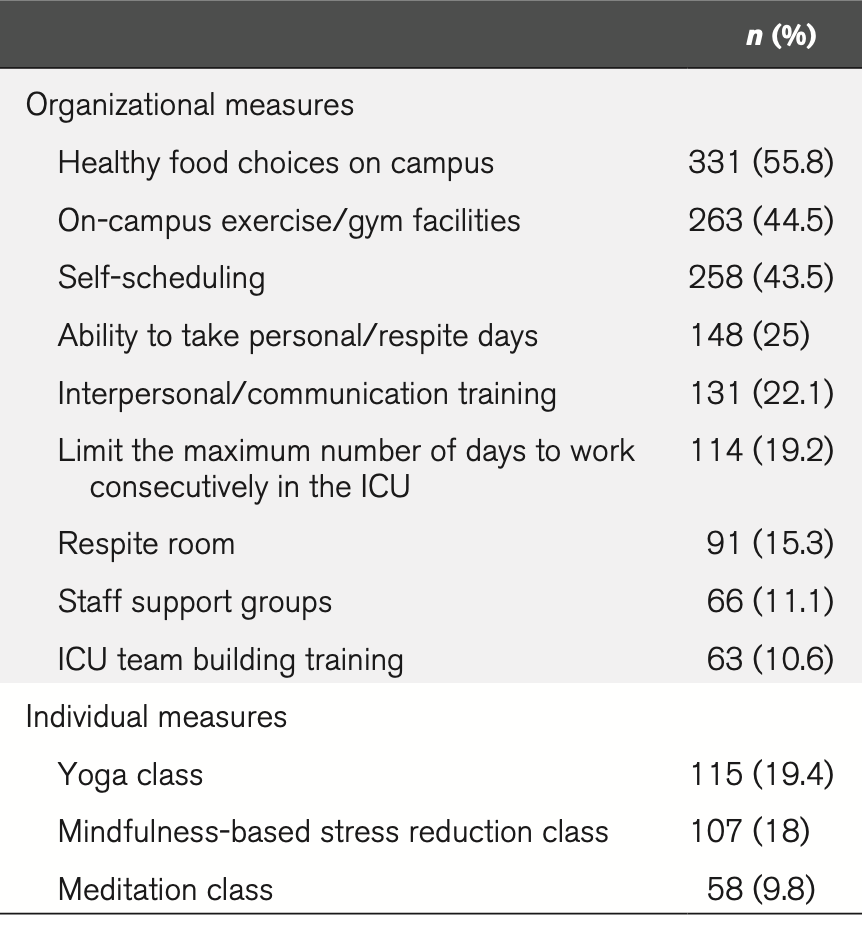
In order to present a tangible solution to the issue of burnout on the ICU premises, the data from the summit and the survey were synthesized with the help of allocating the prevalence of each of the proposed burnout prevention interventions and combining this information with the summit’s educational aspect. Such a combination of the theoretical background, along with the practical application, can provide valuable insights into the future of burnout prevention planning. However, as far as the complexity of studies is concerned, the primary bias concerns the fact that all of the studies were somehow related to the activity of CSSC and its members.
The majority of the analysis authors gained CCSC support during the research, including access to the primary survey data, as survey results are accessible exclusively to the CCSC leadership (Kleinpess et al., 2020). There was no control group of the survey that would answer the same questions based solely on their experience and not CCSC data. For this reason, there was a significant risk of the authors being interested in finding out the relevance of the proposed burnout interventions. No additional analyses were employed throughout the research process.
Results
The study selection for the final research had undergone a series of stages. In the initial statement presented by Moss et al. (2020), the authors used the PRISM approach to detect and analyze studies explicitly related to the burnout syndrome in ICU. In the study in question, for its part, a total of twenty-two sources were utilized, and this reference list included studies outlined in the Moss et al.’s research, such as the studies conducted by Merlani et al. (2011) and Teixeira et al. (2013), the collaborative statement itself, and some of the latest findings on the matter, including research by Dzau et al. (2018) and Panagioti et al. (2017). Along with the studies, the survey findings were utilized. Hence, the flowchart of study selection will look as follows:
As far as the study characteristics are concerned, out of twenty-two resources addressed, ten studies were quantitative and mixed-methods studies on the prevalence and prevention of burnout in the ICU working environment, with samples varying from 200 to nearly 1,000 participants. Some studies, including research by Dzau et al. (2018), are purely qualitative and provide reflexive value to the analysis. When speaking of a survey, it comprised approximately 680 eligible participants that returned their e-mail questionnaires. The survey included six questions that addressed the importance of burnout prevention, awareness levels, and the currently existing burnout prevention techniques employed at the respondents’ workplace (Kleinpell et al., 2020).
No primary studies mentioned in the study had an explicit effect on the outcomes of the analysis, so no individual biases were addressed within the study conducted by Kleinpell et al. (2020). The synthesis of the survey findings and the survey content was presented in the form of a consensus statement that underscored the need for burnout prevention in the case. However, considering the fact that the empirical data were used exclusively from one source, namely, a follow-up survey, no statistical data synthesis was possible in the research.
The result of each individual study, including Moss et al.’s collaborative statement, survey, and studies by Dzau et al. (2018), Merlani et al. (2011), Panagioti et al. (2017), and others, reached the conclusion of a higher burnout risk in such stressful clinical environments as ICUs. Moreover, the results of the intervention groups within the studies recognized the need for physician- and organization-directed interventions such as individual control over scheduling, time-management, and work-life balance education (Panagioti et al., 2017).
Such a unanimous outcome of the studies involved presents the risk of poor critical appraisal of the existing data on the matter. While focusing on the beneficial aspects of burnout prevention, the study does not present an example of a controversial statement that should be refuted. As a result, it becomes evident that the authors did not address the risk of being proclaimed biased. No additional analysis was introduced and addressed in the results of the study.
Discussion
The only unique evidence presented by the present study is the analysis of the follow-up survey results. While the data from the survey were taken from the Project Redcap digital database in order to avoid participant disclosure, the study itself has no verification of these data genuineness whatsoever, as there are no references or images verifying the data extraction. For this reason, even though the findings resonate with the previously published studies by Panagioti et al. (2017) and Merlani et al. (2011), the relevance of the evidence is rather questionable.
This incompleteness, along with biases associated with lack of empirical data, control groups, and one-sidedness of the research, contributes to the limitations of this research. The study did not proclaim explicit funding of any establishment or organization. Still, the authors of the research received much support from CCSC and adjacent organizations, which resonates with the authors’ unwillingness to contrast the follow-up summit survey results with a control group.
References
Dzau, V. J., Kirch, D. G., & Nasca, T. J. (2018). To care is human—collectively confronting the clinician-burnout crisis. New England Journal of Medicine, 378(4), 312-314. Web.
Kleinpell, R., Moss, M., Good, V. S., Gozal, D., & Sessler, C. N. (2020). The critical nature of addressing burnout prevention: Results from the Critical Care Societies Collaborative’s national summit on prevention and management of burnout in the ICU. Critical Care Medicine, 48(2), 249-253. Web.
Merlani, P., Verdon, M., Businger, A., Domenighetti, G., Pargger, H., & Ricou, B. (2011). Burnout in ICU caregivers: a multicenter study of factors associated to centers. American Journal of Respiratory and Critical Care Medicine, 184(10), 1140-1146. Web.
Moss, M., Good, V. S., Gozal, D., Kleinpell, R., & Sessler, C. N. (2016). An official critical care societies collaborative statement: Burnout syndrome in critical care health care professionals: A call for action. American Journal of Critical Care, 25(4), 368-376. Web.
Panagioti, M., Panagopoulou, E., Bower, P., Lewith, G., Kontopantelis, E., Chew-Graham, C., Dawson, S., Van Marvijk, H., Geraghty, K., & Esmail, A. (2017). Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Internal Medicine, 177(2), 195-205. Web.
Teixeira, C., Ribeiro, O., Fonseca, A. M., & Carvalho, A. S. (2013). Burnout in intensive care units-a consideration of the possible prevalence and frequency of new risk factors: A descriptive correlational multicentre study. BMC Anesthesiology, 13(1), 1-15. Web.
