What is readmission?
It is an admission to a hospital during the first 30 days of discharge. It occurs either in the same hospital or another, but due to the same problem. Majorly caused by re-infection of the treated problem. And also ineffective discharge check-up before patients are sent home. Readmissions after major surgical procedures are frequent. It is becoming a problem for most chronic infected patients. Readmissions are emerging as a major problem. They impact an epidemic proportion of urological patients. Readmissions have piqued the interest of major healthcare payers in the United States. Additionally, readmissions have a negative impact on patients’ sense of well-being (Lucas & Pawlik, 2014). The majority of large urologic oncology procedures need readmission during the first two weeks after discharge. This makes it critical to improve symptom identification and readmission rates. Achieving a 0% readmission rate for major surgery is impossible. We must strive to reduce it as much as feasible via effective integrated approaches in order to improve our patients’ care continuum.
Study Objectives – Aim
SPECIFIC: Every year, billions of dollars in needless hospital readmissions are borne by the public, which results in a financial burden on the government. As the era of healthcare reform continues, a growing number of practitioners will be under greater pressure to cut costs and prevent needless and avoidable re-hospitalizations, which will be a source of concern for many (Merkow et al., 2015).
MEASURABLE: However, it is possible to decrease unintentional readmissions to a certain extent by implementing programs that enhance patient care and help patients in moving from one stage of treatment to another across the healthcare system (Deaver et al., 2018).
ACHIEVABLE: As a consequence of the Patient Protection and Affordable Care Act’s (ACA) implementation, hospitals with high 30-day readmission rates are obliged to decrease their Medicare and Medicaid reimbursements to the Centers for Medicare and Medicaid Services (CMS).
RELEVANT: The characteristics and circumstances of a patient may raise their risk of readmission to the hospital within a few days after release. Specific medical / surgical diagnoses, mental health problems, advanced age, a history of readmissions, financial difficulties, and insufficient living conditions all lead to rehospitalization (Deaver et al., 2018).
TIME SPECIFIC: Every day, the healthcare system sees hundreds of thousands of hospital patients. Interactions between patients and healthcare workers occur both during and after a patient’s stay in medical, surgical, or specialized facilities (Lucas & Pawlik., 2014).
Study Objectives – Project Scope
Using risk-standardized readmission rates as a proxy for the number of transitional care operations performed. This study investigated the relationship between the number of transitional care procedures performed and the risk of readmission (RSRR). Hospitals with a high 30-day readmission rate are penalized by Medicare. Numerous clinical trials have shown that a variety of care transition strategies reduce readmissions. New ways to facilitate the adoption of these evidence-based procedures are likely necessary to further decrease readmissions. Given the variability of implementation and the barriers doctors have found to completing activities consistently. Private and Public hospitals should implement the Hospital Readmission Reduction Program (HRRP). Having family, patient seminars, that is for most relevant infections about Homebased care; this will help in the reduction of readmission.
Some underutilized techniques, such as patient participation in discharge planning and more reliance on community resources, should be explored (Lucas et al., 2013). All facilities had inpatient social workers and/or specialist case managers, but many lacked or had limited access to real bridge personnel (following the patient from inpatient to home and even providing home visits). Additionally, additional investment in these roles may be required. The six approaches outlined above will be utilized in conjunction with an overall plan to improve patient care in order to decrease hospital readmissions. Transition of Care models integrates these components into a planned and coordinated hospital program as patients transition from admission to post-discharge. Transition of Care approaches includes multidisciplinary collaboration, education, and communication to provide the best possible inpatient care. In addition, patients get follow-up phone calls or home visits from their primary care physicians as required after discharge.
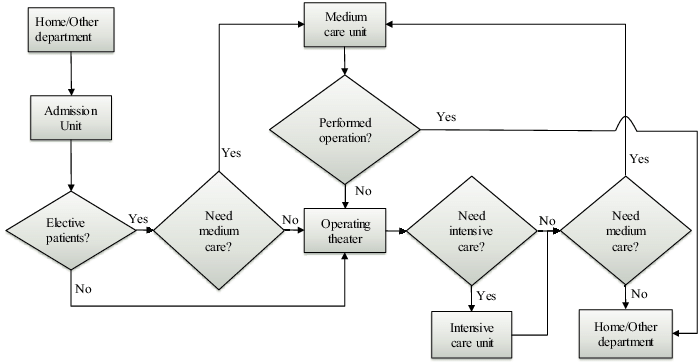
Process Flow Diagram
Surgery Admissions and Re-admissions
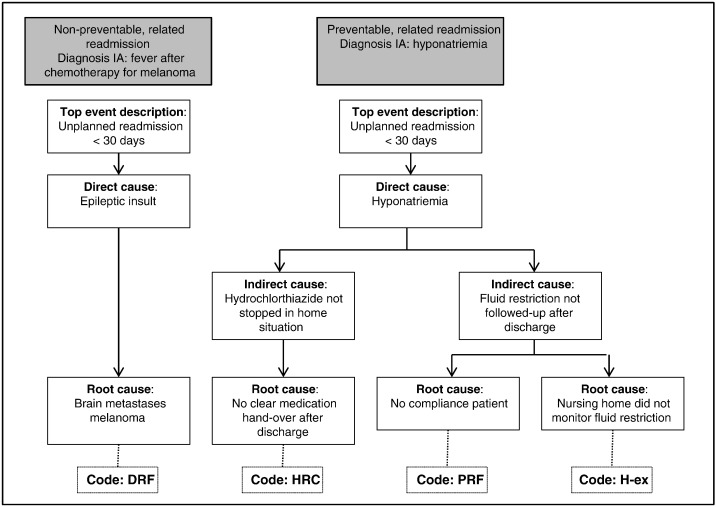
Root Cause Analysis
Surgery Re-admissions
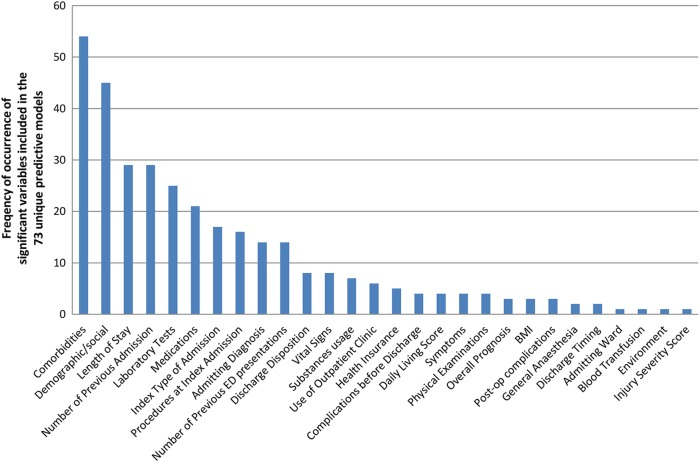
Pareto Chart
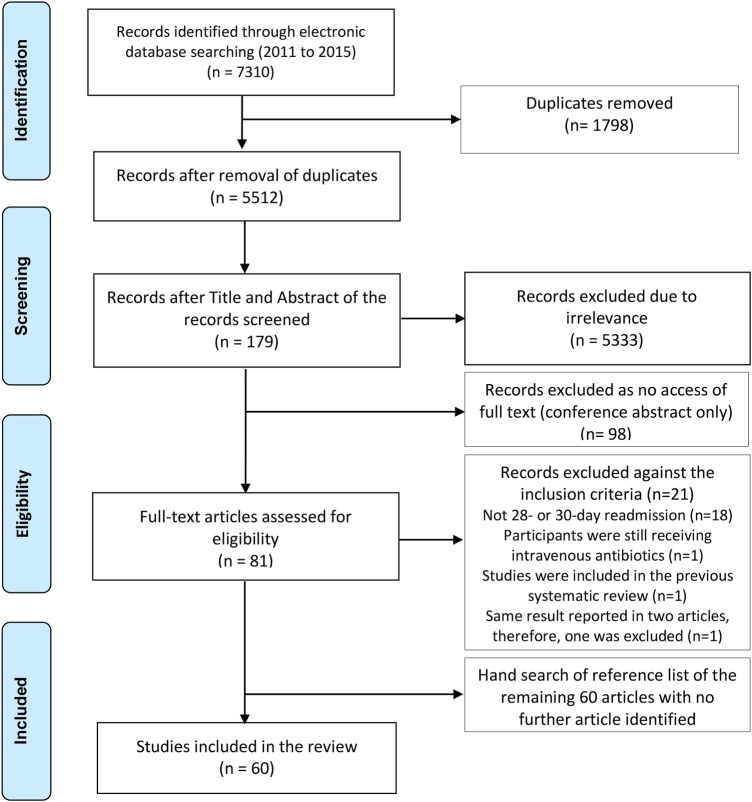
Data Collection for causes from Root Cause Analysis
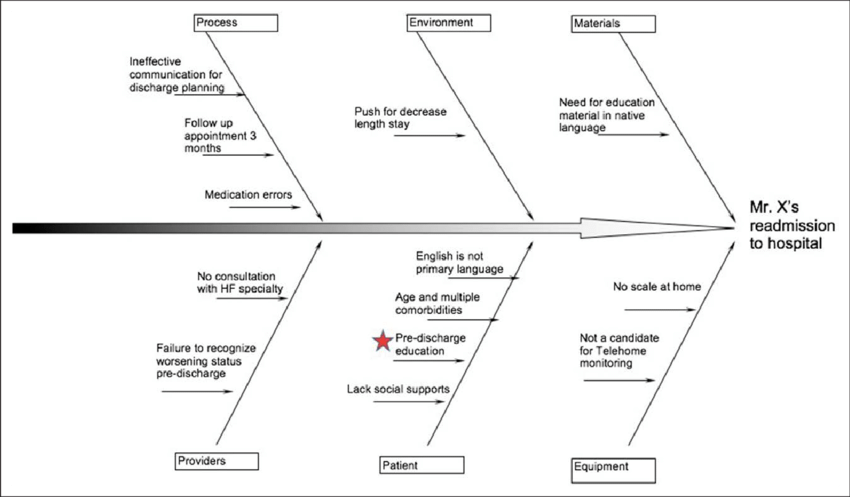
Data Collection for causes from Fishbone
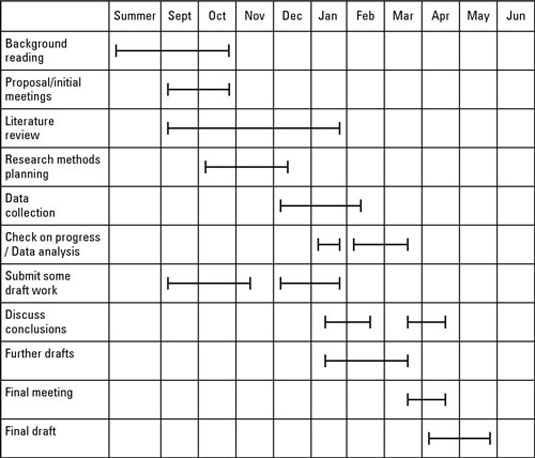
Time Frame for the research
The Chart using the Pareto Rule
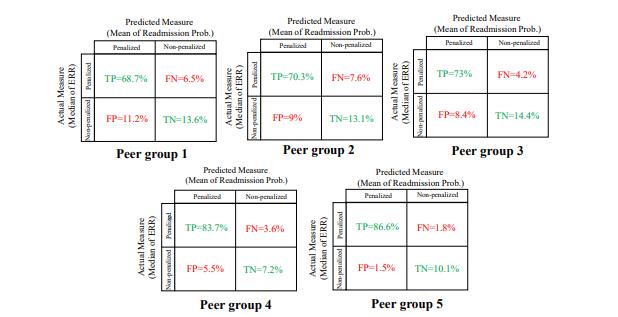
Decision Matrix: List of Solutions
Decision Matrix: Method Used
Decision Matrix: Priorities Based on Average Scores
Next Steps
The problem of people being readmitted after major surgery is a significant one that is increasing. Additionally, they increase the cost of health care while draining the financial resources of patients and their families (Deaver et al., 2018). Furthermore, readmissions will incur financial penalties. It should be a policy that hospitals having a large number of readmissions should be ready for penalties, treat patients under readmission under no charges, i.e. after the cause of the case is investigated. As a consequence, preventing urological readmissions must be a top focus. Cystectomies will continue to be our major area of emphasis for improvement if readmission rates can be successfully decreased. Vascular surgeons face most risks if a patients has a readmission before the proposed time, it opens up for doubt on service provided in the specific hospital. If readmission rates can be effectively lowered, other large enterprises may follow suit and make it safer for most patients with chronic infections other than risking lives (Brooke et al., 2012,). The ultimate aim of minimizing the need for ICU readmissions should be early detection of post-discharge complications. The first one to three weeks after discharge are more likely to provide outcomes. Numerous techniques exist in different areas of medicine that should be used and studied for individuals who have had major surgery. Reviewing evidences that are proposed to identifying risk factors and various intervention on completely fighting readmissions.
References
Babayan, R. K. (2015). Re: Underlying reasons associated with hospital readmission following surgery in the United States. Journal of Urology, 194(2), 448-448. Web.
Brooke, B. S., De Martino, R. R., Girotti, M., Dimick, J. B., & Goodney, P. P. (2012). Developing strategies for predicting and preventing readmissions in vascular surgery. Journal of Vascular Surgery, 56(2), 556-562. Web.
Deaver, K. E., Catel, C. P., Lillehei, K. O., Wierman, M. E., & Kerr, J. M. (2018). Strategies to reduce readmissions for hyponatremia after transsphenoidal surgery for pituitary adenomas. Endocrine, 62(2), 333-339. Web.
Fong, Z. V., Ferrone, C. R., Thayer, S. P., Wargo, J. A., Sahora, K., Seefeld, K. J., Warshaw, A. L., Lillemoe, K. D., Hutter, M. M., & Fernández-del Castillo, C. (2013). Understanding hospital readmissions after Pancreaticoduodenectomy: Can we prevent them? Journal of Gastrointestinal Surgery, 18(1), 137-145. Web.
Hechenbleikner, E. M., Makary, M. A., Samarov, D. V., Bennett, J. L., Gearhart, S. L., Efron, J. E., & Wick, E. C. (2013). Hospital readmission by method of data collection. Journal of the American College of Surgeons, 216(6), 1150-1158. Web.
Lucas, D. J., Haider, A., Haut, E., Dodson, R., Wolfgang, C. L., Ahuja, N., Sweeney, J., & Pawlik, T. M. (2013). Assessing readmission after general, vascular, and thoracic surgery using ACS-NSQIP. Annals of Surgery, 258(3), 430-439. Web.
Lucas, D. J., & Pawlik, T. M. (2014). Readmission after surgery. Advances in Surgery, 48(1), 185-199. Web.
Merkow, R., Ju, M., & Chung, J. (2015). Underlying reasons associated with hospital readmission following surgery in the United States. Journal of Vascular Surgery, 62(1), 265. Web.