Summary
The patient’s admitted medical diagnosis is rapture in the bone in the right hip, a common effect resulting from falls in older adults (Yang et al., 2020). The surgical procedure that was performed to address the condition was a right hip arthroplasty in which the patient’s hip joint was removed, and an implant was placed to address the mobility issues as well as the pain (Anger et al., 2021). The patient has a history of hypertension (high blood pressure), coronary artery disease(impaired blood flow to the heart muscle), degenerative joint disease (joint impairment due to repetitive motions), and osteoporosis (bone tissue damage) (WHO, 2024; Shahjehan, 2023; AAPMR, 2024; National Cancer Institute, 2024). In addition, he has cataracts (clouding in the eye lens) and hearing problems and has undergone a cholecystectomy, which is gallbladder removal (Shiels & Hejtmancik, 2019; Shahjehan, 2023; Hassler, 2023).
Physical Assessment
I would start by establishing a rapport with the patient. As per health goals, I would conduct a general assessment by observing potential physical signs. The step has been linked to more accurate diagnoses as both physical and behavioral signs are considered (Faustinella, 2020).
I would proceed to obtain the vital signs. Namely, I would check the heart rate using a stethoscope, determine the respiratory rate, and measure the blood pressure (Brekke et al., 2019). I would subsequently obtain temperature and oxygen saturation readings using a thermometer and a pulse oximeter.
As the patient has undergone arthroplasty, I would perform neurovascular checks of the right leg and assess his mobility. It is also vital to inquire about potential pain and its intensity, location, and nature. During the respiratory examination, I can observe the rate of respiration and listen to the individual’s lungs to detect abnormalities. During the cardiovascular check, I will auscultate the heart and compare the data with normal measurements (Warriner et al., 2019).
After surgery, it is critical to question the individual about possible changes in GI and urinary function, as challenges can arise. A psychosocial examination will also be conducted as surgical stress can affect one’s well-being (Villa et al., 2020). Namely, I would discuss stress levels as well as anxiety or concerns.
Priorities
First and foremost, a neurovascular examination is critical, as blood flow may have been impaired after surgery. In addition, the possibility of nerve damage can lead to a variety of adverse outcomes for individuals, which can be prevented through the selected assessment. In addition, analyzing the mobility and motion of the right leg is paramount. Potential side effects, such as inflammation, may occur, and appropriate physical therapy can significantly enhance recovery.
The third element is pain assessment, as this aspect may make the individual less mobile and, as a result, recovery will not be achieved in a timely and efficient manner (Turan et al., 2023). Due to the previous history of hypertension and coronary artery disease, the cardiovascular assessment is also included in priorities.
Lung Sounds
Normal lung sounds can be characterized as low-pitched and soft, high-pitched and loud, and a mixture of both, depending on whether they are vesicular, bronchial, or bronchovesicular. In contrast, abnormal ones include crackles, wheezes, and rhonchi (Kim et al., 2021). Crackles are common in patients with pulmonary edema or pneumonia and result from fluid accumulation in the alveoli or airways. Wheezes, on the other hand, are typical of people with asthma or COPD and are caused by narrowing of the airways (Kim et al., 2021). Rhonchi, which correlate with chronic bronchitis, are caused by excessive secretions.
Heart Sounds
Normal heart sounds are heard as the beginning of the systole and diastole and coincide with the closure of the atrioventricular and semilunar valves. Abnormal sounds (third and fourth sounds) are heard in early and late diastole and may indicate specific conditions (Marocchi et al., 2023). The third one may be caused by heart failure and happens as blood fills the ventricles as they relax before the next contraction. The fourth heart sound, which correlates with hypertension, occurs when the atria push blood into a stiff ventricle.
Home Return and Nursing Intervention
It is unlikely for the patient to be able to return home and care for himself. Older patients are more likely to develop new vulnerabilities after surgeries (Shulman et al., 2023). Options to consider include home care services or assisted living facilities. As per nursing interventions, venous thromboembolism, which is common after arthroplasty, can be prevented pharmacologically and through leg elevation, exercise, and mobilization (Al-Mugheed et al., 2023). To minimize the risk of infection, the post-surgical wound is to be treated with antibiotics and with proper antiseptic and hygiene routines. Last but not least, to prevent dislocation, the intervention should include patient education on mobility and physical assistance.
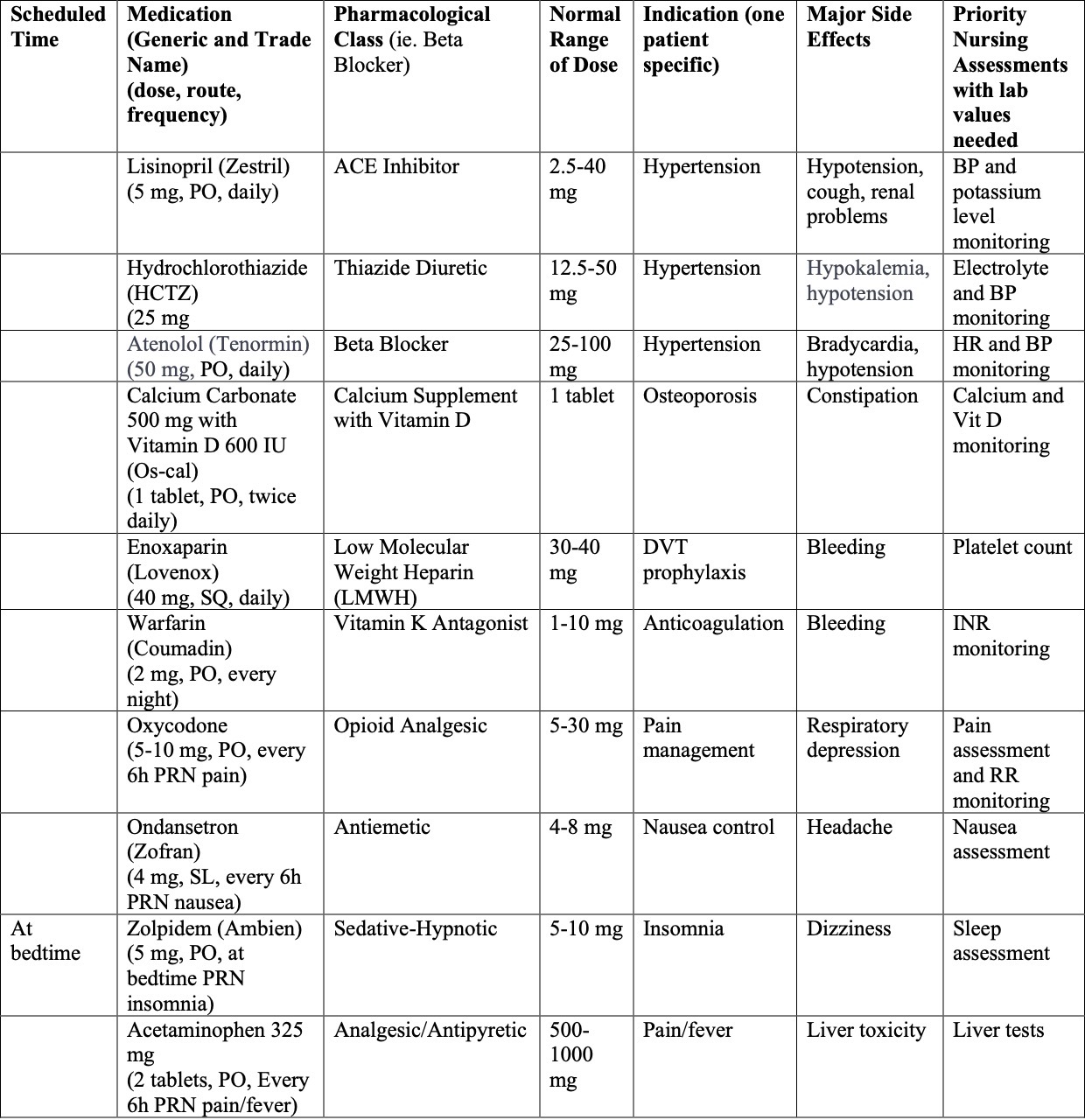
Medication
Warfarin increases the risk of bleeding and requires close monitoring, which is a concern. In addition, respiratory depression is a relatively common occurrence linked to oxycodone administration (Dahan et al., 2022). Similar to warfarin, enoxaparin can increase the risk of blood thinning and bleeding.
References
AAPMR. (2024). Degenerative joint disease. www.aapmr.org.
Al-Mugheed, K., Totur Dikmen, B., Bayraktar, N., Farghaly Abdelaliem, S. M., & Ahmed Alsenany, S. (2023). Nursing care and barriers for prevention of venous thromboembolism in total knee and hip arthroplasty patients: A qualitative study. Journal of Multidisciplinary Healthcare, Volume 16, 547–556.
Anger, M., Valovska, T., Beloeil, H., Lirk, P., Joshi, G. P., Van de Velde, M., & Raeder, J. (2021). Prospect guideline for total hip Arthroplasty: A systematic review and procedure‐specific postoperative pain management recommendations. Anaesthesia, 76(8), 1082–1097.
Brekke, I. J., Puntervoll, L. H., Pedersen, P. B., Kellett, J., & Brabrand, M. (2019). The value of vital sign trends in predicting and monitoring clinical deterioration: A systematic review. PLOS ONE, 14(1).
Dahan, A., van Lemmen, M., Jansen, S., Simons, P., & van der Schrier, R. (2022). Buprenorphine: A treatment and cause of opioid-induced respiratory depression. British Journal of Anaesthesia, 128(3), 402–404.
Faustinella, F. (2020). The power of observation in clinical medicine. International Journal of Medical Education, 11, 250–251.
Hassler, K. R. (2023). Laparoscopic cholecystectomy. StatPearls.
Kim, Y., Hyon, Y., Jung, S. S., Lee, S., Yoo, G., Chung, C., & Ha, T. (2021). Respiratory sound classification for crackles, wheezes, and rhonchi in the clinical field using deep learning. Scientific Reports, 11(1).
Marocchi, M., Abbott, L., Rong, Y., Nordholm, S., & Dwivedi, G. (2023). Abnormal heart sound classification and model interpretability: A transfer learning approach with deep learning. Journal of Vascular Diseases, 2(4), 438–459.
National Cancer Institute. (2024). NCI dictionary of cancer terms.
Shahjehan, R. D. (2023). Coronary artery disease. StatPearls.
Shiels, A., & Hejtmancik, J. F. (2019). Biology of inherited cataracts and opportunities for treatment. Annual Review of Vision Science, 5(1), 123–149.
Shulman, M. A., Wallace, S., Gilbert, A., Reilly, J. R., Kasza, J., & Myles, P. S. (2023). Predicting death or disability after surgery in the older adult. Anesthesiology, 139(4), 420–431.
Turan, A., Khanna, A. K., Brooker, J., Saha, A. K., Clark, C. J., Samant, A., Ozcimen, E., Pu, X., Ruetzler, K., & Sessler, D. I. (2023). Association between mobilization and composite postoperative complications following major elective surgery. JAMA Surgery, 158(8), 825.
Villa, G., Lanini, I., Amass, T., Bocciero, V., Scirè Calabrisotto, C., Chelazzi, C., Romagnoli, S., De Gaudio, A. R., & Lauro Grotto, R. (2020). Effects of psychological interventions on anxiety and pain in patients undergoing major elective abdominal surgery: A systematic review. Perioperative Medicine, 9(1).
Warriner, D., Michaels, J., & Morris, P. D. (2019). Cardiac auscultation: Normal and abnormal. British Journal of Hospital Medicine, 80(2).
WHO. (2024). Hypertension. World Health Organization.
Yang, Y., Komisar, V., Shishov, N., Lo, B., Korall, A. M., Feldman, F., & Robinovitch, S. N. (2020). The effect of fall biomechanics on risk for hip fracture in older adults: A cohort study of video‐captured falls in long‐term care. Journal of Bone and Mineral Research, 35(10), 1914–1922.
Appendix
Table 1 – List of Prescribed Medications