When dealing with illness in a family, nurses are challenged with applying properly designed tools, strategies, and interventions that would suffice the needs of an individual and the family. Indeed, the family-centered approach to nursing allows for an integrative methodology and practice of healthcare, in which the immediate environment, in which a patient lives, is actively involved in the process of healing. According to the Calgary Family Assessment Model (CFAM) and Calgary Family Intervention Model (CFIM), health and treatment should be addressed in the context of the capacity of family structure and functioning to affect the health of its members (Leahey & Wright, 2016). Therefore, for the purposes of this family case study, CFAM will be used to assess the family, and CFIM will be used to generate interventions to address the family’s concerns and yield anticipated outcomes. According to Leahey and Wright (2016), CFAM implies the evaluation of families according to three aspects, namely structure, functioning, and development.
From the structural perspective, the family is assessed and described as per the number of units or members in it, their relations, occupations, and the interaction with a larger social context. The family chosen for the case study is a family of two, Peter Jones (PJ), aged 57, and his wife Anne Jones (AJ), aged 55. The couple has one child, a daughter Julia (JJ), who now has her own family, lives in another city and is not involved in the family matters between her mother and father. The issue at the nurse’s hand is the recent diagnosis of PJ with prediabetes and his reluctance to adhere to the recommended lifestyle changes and dieting for the minimization of diabetes risk.
Thus, in terms of the internal structure, the family consists of two individuals; AJ works as a teacher at school, and PJ is an electrician. They both are in their pre-retirement stages employment-wise; however, they actively participate in professional lives and remain socially participative in their community. Within the CAFM, the structure is subcategorized into internal (nuclear family) and external (extended family) structures (Leahey & Wright, 2016). The external family structure involves AJ’s two brothers and PJ’s sister, who live in the neighborhoods nearby and visit occasionally. Both parents of both spouses of the family are deceased. From an economic stance, the family is considered middle class with their salaries covering their monthly bills and daily needs for food, medication, and other essentials. The family owns a house in a rural area and a car.
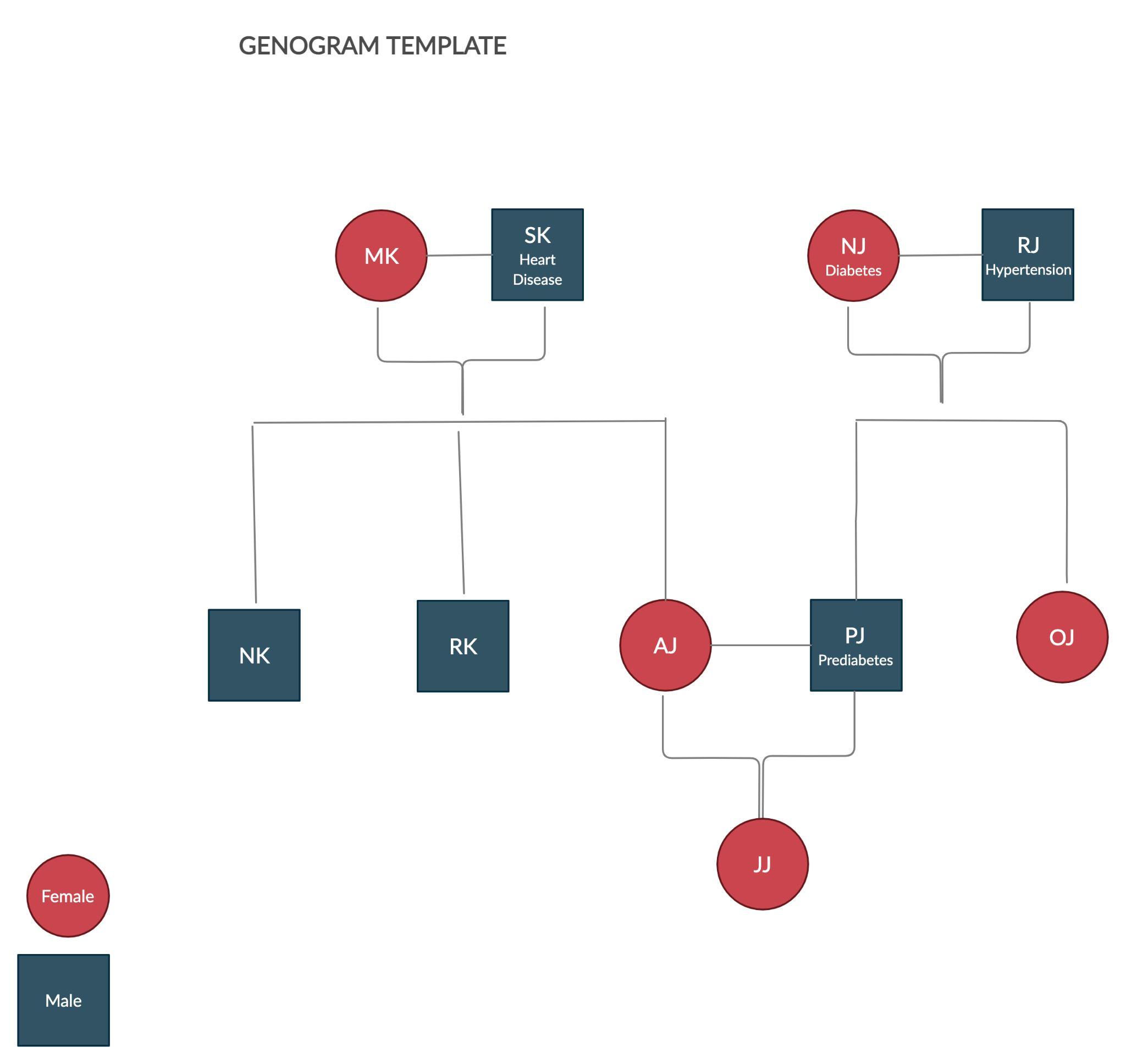
At the stage of family assessment, a nursing practitioner might use a genogram, which is an effective tool that reflects the interrelations between family members and their health. It is commonly represented in the form of a scheme with the genealogy of a family displayed in the form of branches and units. According to Turabian (2017), this tool provides nurses with essential data necessary for making conclusions about health concerns prevalent in the family and the potentially applicable techniques of overcoming them. Genograms are applicable for a variety of purposes due to the versatile data it might reflect, including “family structure, life cycle in which that family is, important vital events, family resources, relational family patterns” and other details essential for family-centered care (Turabian, 2017, p. 187). The genogram created for the Jones family demonstrates the parents and siblings of each of the spouses and their child (Figure 1). Family health history reflected in the genogram demonstrates that PJ has a high level of risk of developing diabetes due to his mother’s history of diabetes and his father’s hypertension, which also might have a negative effect on the patient’s health.
From the functional point of view, the family members’ interaction, emotional responsiveness to each other, communicational ties, and other particularities are measured. According to Lavorgna et al. (2020), the Dyadic Adjustment Scale, which was “developed to evaluate marital relations,” is a valuable tool for assessing functionality (p. 2). According to this scale, the couple faces challenges achieving agreement in controversial opinions, including the necessity of PJ to change his lifestyle, quit smoking, be more physically active, and keep to a healthy diet. As for the emotional aspect of family functionality, the family displayed a high level of mutual support, compassion, and empathy. They participate in most daily activities together, although PJ has recently been reluctant to join AJ in shifting to healthier meals and walks in the evening. In addition, the assessment showed that both spouses demonstrate a moderate level of satisfaction with their partner. Therefore, the most problematic aspect that prevents the family from proper functioning and causes difficulties in satisfaction and participation is the disagreement concerning PJ’s health status, which might be validated by PJ’s stress due to elevated health concerns.
As for the level of family development, the coupe might be characterized as the one in the transitioning phase from one stage to another. In particular, as suggested by Kaakinen and Webb (2017), Duval and Miller’s traditional family life cycle approach might be used to assess the level of family development. Accordingly, PJ and AJ are in the transition from the stage of middle-aged parents to aging parents, which implies such family struggles as adjusting to change in health, maintaining kinship ties, refocusing on couple time, and concentration on the future and retirement (Kaakinen & Webb, 2017). Each of the family members is at their normal stage of individual development consistent with their age and position in life. Thus, the assessment of the family shows diminished communicational functioning, participation in daily activities, and satisfaction, all rooted in the couple’s disagreement concerning PJ’s health-improvement practices’ necessity. To address the identified issues, several family theory-informed interventions might be proposed.
Application of Theory to Family Case Study
The interventions proposed for the presented family case will be informed by CFIM, which is an integrative system of tools and intervening methods designed for proper addressing of family concerns. According to Wright and Leahey (1994), “GFIM provides a means to conceptualize a fit between the domains of family functioning and interventions offered by the interviewer” (p. 384). According to this theory, intervention selection and implementation should be meticulously informed on the basis of family assessment. In particular, a nursing practitioner should start by answering the question concerning the agreed problem that necessitates a solution (Wright & Leahey, 1994). In the case of AJ and PJ, the agreed-upon issue is the lack of communication and participatory agreement between husband and wife in terms of health-improving practices aimed at eliminating prediabetes in PJ. Further, the model suggests considering particular family functioning domains involved in the problem-solution process (Wright & Leahey, 1994). The case assessment showed that the couple faces complications in such functional domains as communication, satisfaction, and participation. Given the complexity of the situation, all three domains of family functioning, including cognitive, affective, and behavioral, will be integrated when developing interventions (Wright & Leahey, 1994). Moreover, when selecting interventions, a nurse should consider if they match the family’s style of relating, ethical, and religious beliefs (Wright & Leahey, 1994). Thus, using CFIM guidelines and tools, one might use circular and linear questions for interviews and therapeutic conversations. Some activities might align with the family’s history of successful strategies since the couple is likely to spend time together. Moreover, it is essential to address the family’s difficulty in avoiding stress in communication. These elements will be addressed by specifically designed family-centered interventions that would focus on both family functionality and PJ’s health condition.
Interventions: Family Meetings for Therapeutic Conversations
Among many available interventions in family-centered nursing, the Jones family might benefit from those matching their strengths and addressing their weaknesses. In particular, the first intervention proposed for the couple is the arrangement of family meetings with a health practitioner for a therapeutic conversation. Since one of the main concerns in the investigated case is the lack of understanding and agreement between the family members, the primary goal of the therapeutic communication is to apply interviewing techniques proposed by CFIM to establish common ground. In the course of the conversation, the nurse might use linear, circular questions, opinion retrieval, externalization of the problem, eliciting of behavioral patterns, and hypothesizing about the future (Wright & Leahey, 1994). These techniques will emphasize the ability of the couple to deal with challenges as informed by the history of their marital life and their emotional bond. Moreover, another strength of the family, namely the spouses’ common interests and participation in the same daily activities, will also be used as the basis for problem-solving.
In such a manner, the nurse will be able to help PJ recognize the implications of his health on family relations and the capability of family support to assist him with health improvement. This therapeutic conversation will help Peter look at his prediabetic condition from a perspective of the family’s strengths to eliminate stress and anxiety associated with the fear of diagnosis and concentrate on the solutions to the problem. As for his wife, she will obtain an opportunity to share her opinion about the issue and come to an agreement and communicative compromise with her husband. Despite the solution to the couple’s communication crisis, the therapeutic conversations will address some prediabetes-specific issues. In particular, the nurse will discuss some essential practices and routine activities for healthier blood sugar levels, monitoring, smoking cessation, physical activity, and diet. In such a manner, cognitive and affective domains of family functioning will be addressed by this intervention. Thus, at the initial step of the interventions, the work with the family will be oriented at addressing the main concern, identification of strengths and effective solution routes, as well as outlining an action plan. The anticipated outcomes of this intervention include the elimination of conflict and stress in communication in the family, decreased level of anxiety associated with the prediabetes diagnosis, identification of the common problem, and the understanding of the necessary steps toward its solution.
Couples’ Cooking Classes
The second intervention applicable to the family case is cooking training with the involvement of family members. In this particular case, Peter and his wife will attend courses in cooking where dietitians will give lectures and hold practical classes. This intervention is highly effective in family-centered therapy since family members are “invited to participate in a cooking demonstration by a dietitian to show how to cook healthy meals that are easy and taste good” (Baig et al., 2016, p. 96). This intervention is based on the use of the couple’s strengths inherent in their appreciation of time spent together and in their shared participation in activities. Therefore, by means of cooking classes attendance, the Joneses will address the problem of the lack of knowledge and a unified direction in prediabetes management by means of adjusting their dieting toward desired goals. As a result of this intervention, cognitive and behavioral domains of family functioning will be addressed; the family is anticipated to obtain knowledge and skills in preparing healthy meals using whole foods and diabetes-friendly nutrients. Moreover, as a family, they will eliminate conflict, improve communication effectiveness, enhance emotional ties, and create a solid basis for Peter’s healing.
Educational Therapy for Prediabetes Management
The third intervention that might be effective for the family in the case study is educational therapy for prediabetes management. In this therapy, the involvement of a family member will play an essential role since the support of patients contributes to consistency and success in healthy behavioral pattern acquisition. Studies show that “among adults, the inclusion of a close family member in psychosocial interventions for chronic conditions may also be more efficacious than focusing solely on the patient” (Baig et al., 2016, p. 93). Indeed, evidence demonstrates that educational interventions in which patients participated with their close family members yielded improved “rates of smoking cessation and weight loss” (Baig et al., 2016, p. 93). It implies better outcomes in comparison to the results obtained from interventions held for patients without family members’ inclusion.
Educational therapy for prediabetes management will inform the patient and his wife on effective strategies of stabilizing the health condition, using apps to monitor blood sugar, set physical activity goals, design strategies to quit smoking, and other essential elements. According to Wright and Leahey (1994), behavioral change is essential in family-centered interventions. For that matter, the family should be encouraged to initiate some family rituals and new household habits that would assist their effective communication and help them manage Peter’s prediabetes consistently. For example, the couple might initiate daily night-time conversations expressing concerns and worries to each other and expressing support. Such a ritual will build enhanced trust, emotional bond, and satisfaction in the family, thus creating a favorable environment for improved health outcomes. Thus, the anticipated outcomes of this intervention are the improvement of knowledge of the condition, improved emotional and communicational connection between the spouses, and change in their behavior in terms of dieting, bad habits, and exercising. It will address behavioral and cognitive domains of family functioning.
Reflection
When working on this case study, I was able to explore and apply family theories and models, which was a valuable professional experience. The assessment of the family using CFAM provided me with a chance to see the scope of factors that affect patients’ health due to their life as a family unit participating in complicated structures and relations. However, despite this complexity, I managed to organize the information necessary for assessment into domains using specifically designed tools. Similarly, at the stage of intervention development and selection, I applied CFIM, which proved to be an integrative and effective model justifying through-through and informed problem-solving. Given these instruments, I will be able to deliver family-centered care professionally and confidently in my future practice since I have answers to all questions inherent in the abundance of tools and models.
References
Baig, A. A., Benitez, A., Quinn, M. T., & Burnet, D. L. (2016). Family interventions to improve diabetes outcomes for adults. Annals of the New York Academy of Sciences, 1353(1), 89-112. DOI: 10.1111/nyas.12844
Kaakinen, J. R., & Webb, J. F. (2017). Family development and family nursing assessment. In M. Stanhope and J. Lancaster (Eds.), Foundations for Population Health in Community/Public Health Nursing E-Book (pp. 294-309). Elsevier Health Sciences.
Lavorgna, L., Di Tella, M., Miele, G., De Mercanti, S. F., Streito, L. M., Perutelli, V.,… & Clerico, M. (2020). Online validation of a battery of questionnaires for the assessment of family functioning and related factors. Frontiers in Psychology, 11(771), 1-9. h
Leahey, M., & Wright, L. M. (2016). Application of the Calgary Family Assessment and Intervention Models. Journal of Family Nursing, 22(4), 450–459. doi:10.1177/1074840716667972
Turabian, J. L. (2017). Family genogram in general medicine: A soft technology that can be strong. an update. Research in Medical & Engineering Sciences, 3(1), 186-191.
Wright, L. M., & Leahey, M. (1994). Calgary Family Intervention Model: One way to think about change. Journal of Marital and Family Therapy, 20(4), 381–395. doi:10.1111/j.1752-0606.1994.tb00128.x