Introduction
Modern healthcare is based on continuous improvement processes to address this system’s critical challenge, namely, to provide quality and affordable clinical services to patients. The healthcare system may turn to community profiling tools, the essence of which is to identify the characteristics of a particular region to provide more personalised clinical services to residents. The point of such personalisation is to minimise disparities in health outcomes and access to health support potentially faced by racial, ethnic, and socioeconomic cohorts (Schork, 2019).
In more detail, profiling should be understood as collecting, analysing, and interpreting information about a community to understand its health status, key needs, and necessary resources to achieve well-being (Bhaumik et al., 2020). The information collected and analysed is crucial in the context of an improving healthcare system for providers and decision-makers when designing practical interventions. Community profiling is fundamental to identifying disparities in clinical access, addressing such disparities, planning and delivering the most optimised and effective services to local populations.
The geographical region explored in this essay is a real English community named Ward X in the paper for privacy purposes. Ward X is a small region with a low population and predominantly working adults. The motivation for choosing this domain is not coincidental, as research demonstrates that unhealthy habits are more prevalent in regions with low populations (Buettner-Schmidt et al., 2019). Thus, the selected Ward X community could be considered vulnerable due to the problems inherent in low-population regions.
In addition, the choice of this community is justified by supposedly simpler analysis and intervention schemes, as the lower the population size, the easier it is to make decisions and monitor the effectiveness of implemented changes. It was interesting to look at the context of health and demographics compared to national data from England, and hence to situate Ward X in the midst of national data. In other words, communities like this need to pay as much attention to the health system as possible to identify critical patterns and develop appropriate programmes that increase clinical well-being among residents.
This assignment requires professional and academic skills. As a researcher, within this assignment, I exercise my competencies in searching and critically analysing information, citing carefully and structuring thoughts at an academic level (US, 2021). As a professional, I am educated in public health. I know what adequate public health practice should be, how to use resources more effectively, and what community problems can arise (NHS, 2021). As a student of this practice, I can contribute to this process of community profiling through my understanding of the phenomenon of community healthcare.
This essay focuses on Ward X community profiling and coherently explores selected aspects of this analytical process. It includes an extensive review of community demographic and socioeconomic characteristics and determinants of health. The statistics on each parameter presented in the essay are based on facts and evidence published on governmental and authoritative websites. Critical analysis of these data is noteworthy as it provides information on the status of individual determinants of health in the community, which can be used to identify potential needs.
Geographical Area
Ward X has been chosen as the region of interest for this critical analysis. Figure 1 shows the approximate location of this community, which is located in the suburb of Coventry, in the West Midlands region of England. Ward X has an area of 4.689 km2. The principal boundaries of this community are Bell Green and Henley Green, and the region has a rather old history dating back to the Middle Ages. Although Ward X is a reasonably small agglomeration with a low population, the region’s main amenities include many shops, including supermarkets, several parks, and open spaces. There are several community centres and local schools in the area.

Regarding transport connectivity, Ward X offers moderately developed highways to locals, including the A45 and A46 interchanges, municipal transport, and commercial carriers, enabling travel both within the region and between neighbouring agglomerations. Ward X has no city-forming enterprise and industry; there are predominantly retail and services, although small warehouses exist. Thus, regarding geographical location, the Ward X area map has shown it to be a relatively small area in northwest Coventry, not highly developed in an urbanist sense, but presenting moderate transport and industrial opportunities for residents.
Data Analysis
Population Size
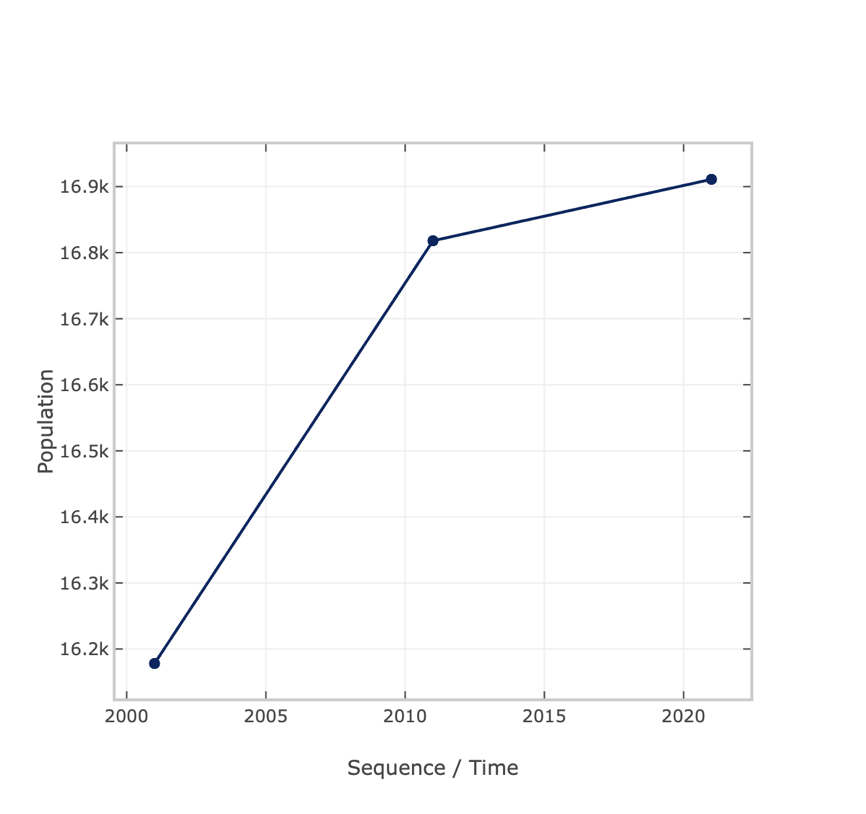
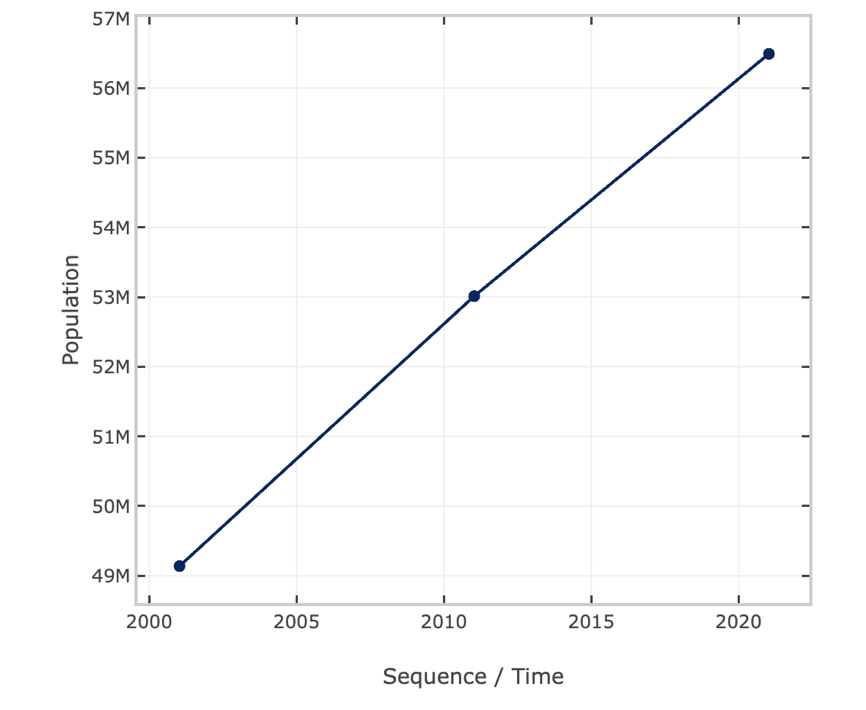
Ward X is a small suburb of Coventry, with a population of 16,911 as of 2021 (CityPopulation, 2021a). Figure 1 shows the statistics for changes in this parameter over the three reporting years, and the overall conclusion is that the population has not changed particularly much over the last twenty years, being in the range of 16,000 to 17,000 people, with a steady increase over this period. For the national data, the pattern holds (Figure 3), and the total population as of 2021 is 56,490,048 (CityPopulation, 2021b).
Population density is an essential indicator for research practice, as studies have reported that this parameter can predict epidemiological patterns in a community (Hamidi and Hamidi, 2021; Sá, 2020). The population density of the region is 3,606 people per square kilometre. Ward X cannot be classified as a rural area but is not a densely populated region (Eurostat, 2021). Furthermore, the total number of households specific to this region is 6,822 as of 2011, and the average local household size is 2.40 (UK Census Data, 2022b). Thus, the population size of the selected community allows it to be considered a typical suburb of a major city (Coventry).
Age Profile
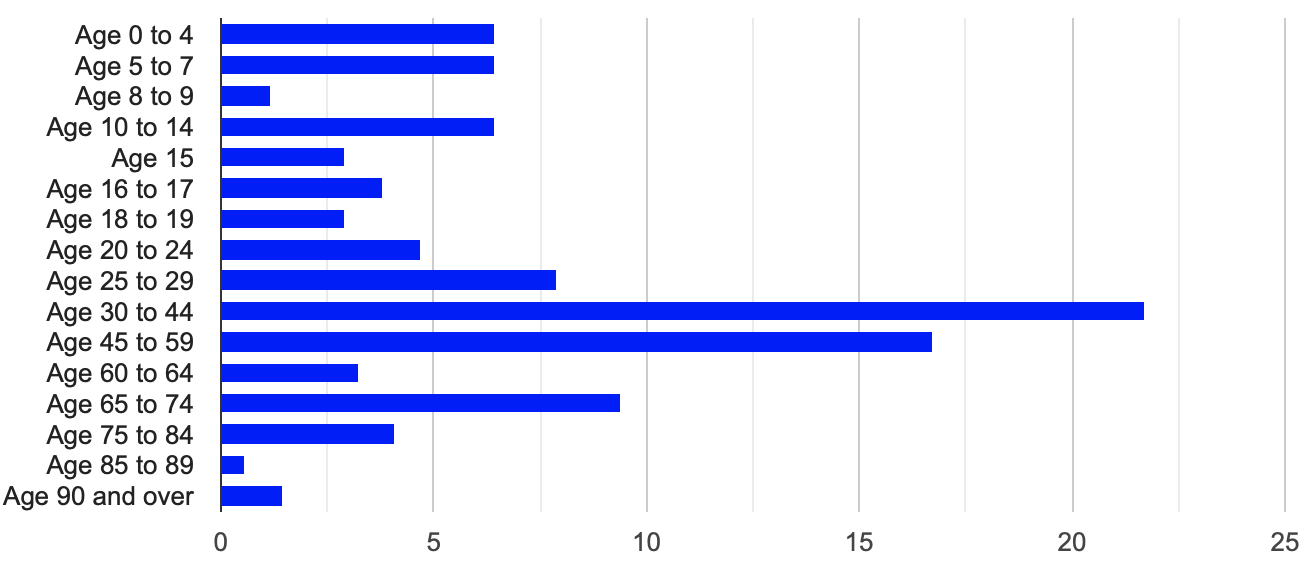
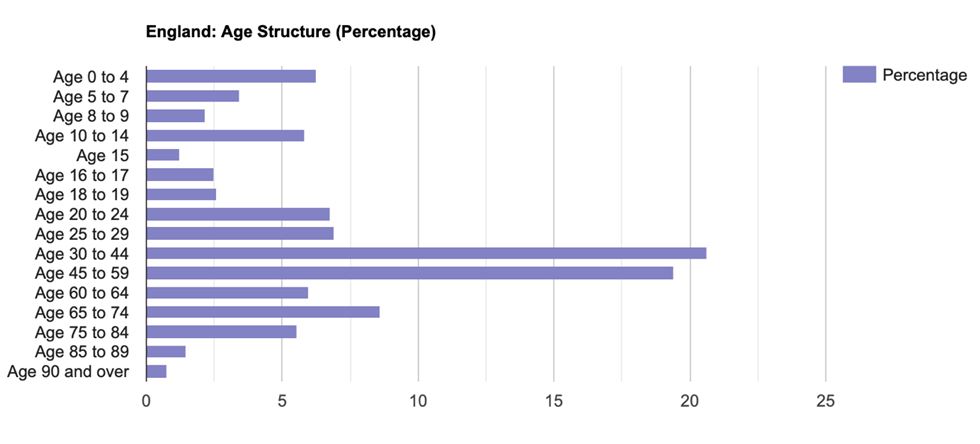
The median age in Ward X as of 2011 was 39, and the median was 38 (Qpzm, 2021). More detailed statistics — as shown in Figure 4 — show that the typical pyramidal formula does not characterise the age distribution of Ward X, and the proportions of the population of different ages did not have a pattern. Nevertheless, the age distribution of the oldest groups is expected to be significantly lower than that of other groups, indicating a reduced need at the community level for palliative and clinical support for older people compared to younger cohorts. However, the picture of national statistics in this dimension (Figure 5) does not differ much from the community level, with the only difference being that the national age group of 15-year-olds is lower in percentage terms than the same community group.
Gender Distribution
Gender determinants are significant in planning health services, as men and women often have different health needs and experiences (Mauvais-Jarvis et al., 2020). According to the 2011 census, the total male population in this region was 49% (n = 8,241) versus 51% for females (n = 8,577), according to Qpzm (2021). For 2021, the gender statistics are unchanged: 48.9% male (n = 8,634) versus 51.1% (n = 8,277) (CityPopulation, 2022). This difference can be seen as absent, which means there is no difference between the numbers of men and women in Ward X, a pattern consistent over ten years. Interestingly, this statistic did not differ from the national statistic, as 49.2% in England were male and 50.8% were female (Nomis, 2011b).
Life expectancy for women in this community is 85 years, and for men, about 77 years, which implies that men, on average, live eight years less in this community than women as of 2006 (CCC, 2022). In the national context, these figures are 79 years for men and 83 years for women, which differ from the local statistics. Three conclusions emerge from this: firstly, there is an increased need for clinical support for older men in the Ward X community, as their life expectancy is lower. Secondly, single widows living in Ward X may require clinical and psychological support (ONS, 2021). Thirdly, the variation in national data may show that not all national programmes can be effectively applied at a community level.
Ethnicity
As it is known that some ethnic groups may be more vulnerable to disease than others, consideration of ethnic statistics is critical to community profiling (Hooper, Nápoles, and Pérez-Stable, 2020). Figure 6 shows that the dominant ethnic group (79%) for the region is White, with Others being the least represented (1%) (Nomis, 2011a). The majority of clinical services should be aimed at White residents of the community, but this does not mean that service offerings to other ethnic groups should be limited.
The moderate representation of other ethnicities in the community suggests that the healthcare system should consider them and offer them appropriate services of decent quality. From a national perspective, the community pattern found is confirmed, although the representation of White at the national level is much higher (Nomis, 2011b). Despite the representation of ethnic groups in Ward X, there is little presence of special themed facilities, religious representations, places of worship, and ethnic shops in the region. The absence or under-representation of ethnically specific facilities can be a problem, especially considering religious statistics. For example, the majority of Ward X (50.2%) is Christian, but Sikh (6.3%), Muslim (4.3%), and Hindu (4.6%) are minorities, according to CityPopulation (2022a).
Education Statistics
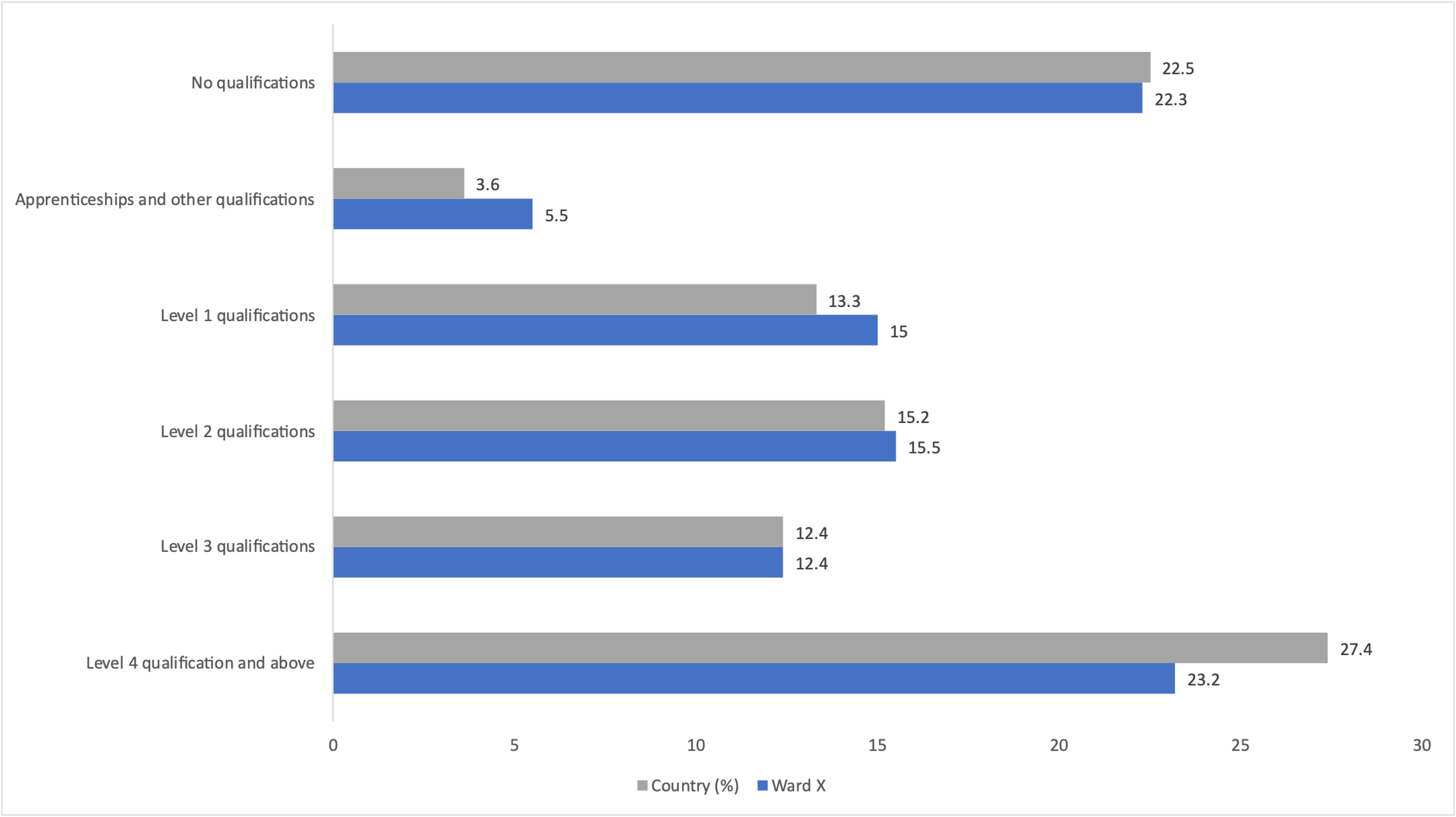
It is known that people with higher levels of education tend to have better health outcomes and lead healthier lifestyles than people do predominantly because they are more likely to have access to information and resources (Stømer et al., 2019). Thus, any community should strive to increase the general level of education, as this will have a favourable effect on health. Figure 8 shows a comparison of the educational attainment of the population at the community and national levels.
There are more people with apprenticeships and first and second-level qualifications in Ward X, but fewer in the other categories. Ward X has fewer, more highly qualified residents than the country (OGL, n.d.). However, it means that Ward X has slightly fewer unskilled residents. Overall, the findings suggest that Ward X has a less educated population than nationally, so the community should try to reach out to the uneducated population, increasing their clinical literacy, and encourage patient education.
Employment
Employment is vital in determining a person’s overall health and well-being. For example, employed and particularly highly skilled people have higher incomes, which causes better healthcare access (Dawes, 2020). Moreover, people often have an institution of socialisation and an environment of peers, strengthening their social identity. In contrast, unemployment can predict serious internal problems, leading to physical ailments (Sarangi, Kim, and Rafael, 2022). As shown in Figure 9, economic activity, defined as employment or job seeker status, is higher for the Ward X community and lower for national data, meaning that people in this region are generally more likely to be active in the labour force.
Figure 10 shows the breakdown of Ward X’s economic well-being by category. This chart shows that the proportion of part-time, full-time, and unemployed people in Ward X is higher than the national statistics. It may follow that decision-makers should adjust federal programmes for employed people and provide clinical support for the unemployed.
There is no available data on the region’s largest manufacturers, probably because Ward X is a suburb, and the main jobs are in neighbouring Coventry. However, as of 2011, the main occupations locally are Professionals (17.34%), Elementary (13.28%), Administrative and secretarial (13.25%), Associate professional and technical (11.07%), and Skilled Trades (10.74%) (Vinsights, 2021). Vinsights (2021) reports that HumanHealth (17.78%), Wholesale (17.06%), and Manufacturing (11.67%) are the critical occupational areas.
Housing Statistics
A large number of homeless people increases the epidemiological disadvantage of the region, so the authorities must look into the affordability of housing. The average price per square foot for Ward X is £252 for 2023; for England, this equates to £282 (Zoopla, 2021; Varbes, 2023). For property in possession, as indicated in Figure 11, “Owned with mortgage or loan” and “Owned outright” are more common in Ward X, in contrast to national data. This may indirectly point to the greater wealth of Ward X compared to the average population in England. Figure 12 supports this conclusion, as Ward X has about twice as many people owning a Whole house or bungalow with a terrace compared to the national data. Thus, the Ward X community predominantly comprises privately owned houses, either directly owned or mortgaged.
Transport
Ward X is linked to several major motorways and allows tourists and residents to travel by car to Coventry in around 10-15 minutes (4.6 km). The community has public transport and nineteen bus stops, allowing residents to move around the region almost seamlessly. Ward X can be reached from Coventry by public transport: buses no. 20, no. 8, and no. 9 connect the agglomerations. Figure 13 shows that Ward X has a higher prevalence of owning one or two cars per household than the national data. This may indicate that Ward X is a typical suburb not characterized by high economic prosperity, and each household has an average number of cars.
Environmental Issues
Little is known about Ward X’s environmental situation, but news sources sometimes report the spontaneous formation of city dumps due to employee strikes (de Souza, 2022). Ward X is a rich ecological reserve with its own central eco-park. At the same time, the area is at risk of flooding and groundwater erosion (OGL, 2023).
Morbidity
According to Figure 14, among the most common chronic diseases, only diabetes is more common in Ward X than the national average. Diabetes is a disease in which the body is unable to use and store glucose properly; a determinant of health, as it can lead to severe complications such as heart disease, kidney failure, blindness, and amputation (Bombak et al., 2020). Among the predictors that can cause diabetes in Ward X (compared to national statistics) are smoking and obesity, which are more represented in Ward than the national average (Figure 15).
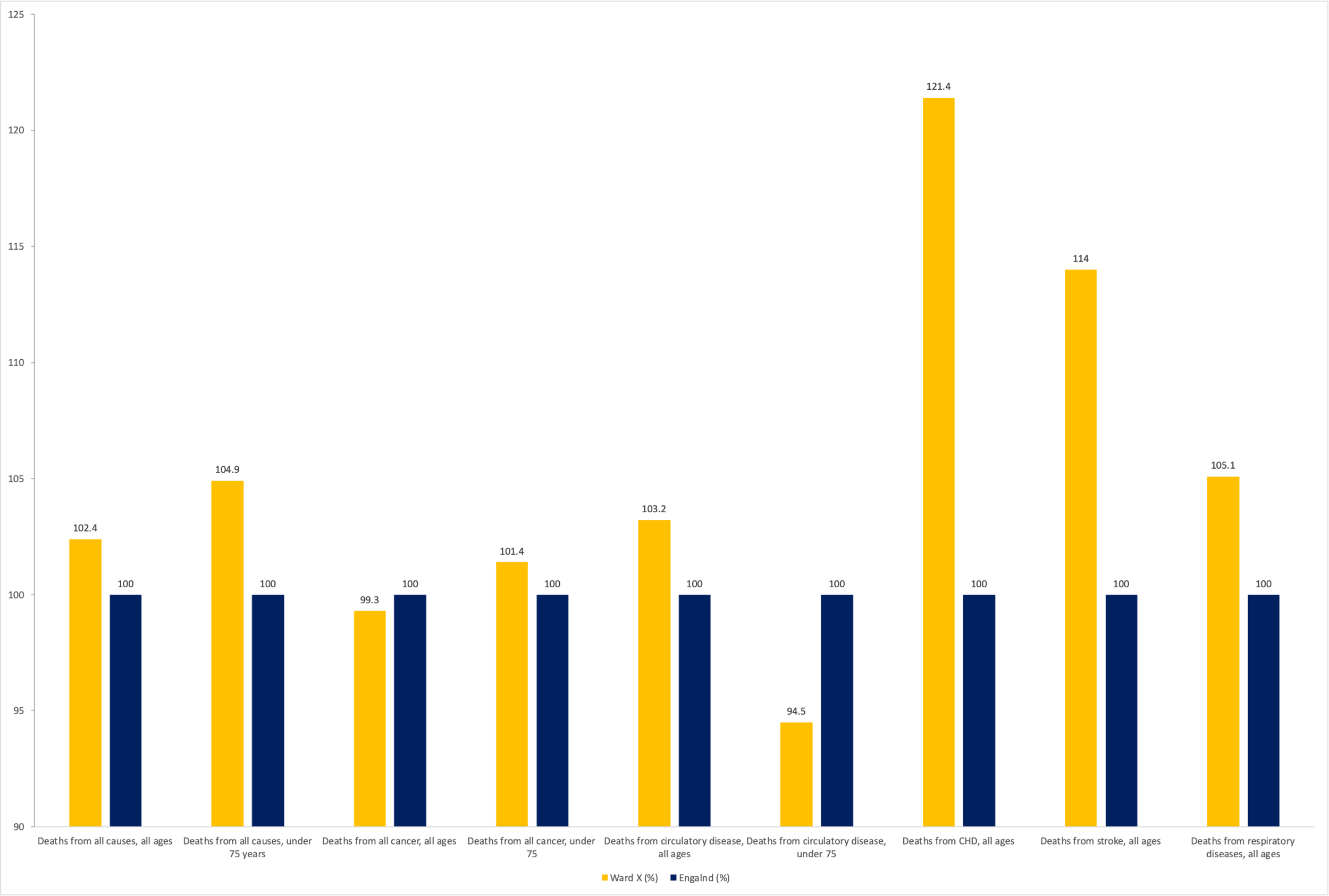
Mortality
Figure 16 shows the leading causes of mortality in the wards in comparison: it can be seen that mortality overall, as well as mortality from all cancers after under 75, cardiovascular disease, CHD, stroke, and respiratory disease, is higher in Ward X. A prominent result is demonstrated for CHD, indicating an increased mortality of people under 75 from this disease. In the context of the prevalence of diabetes defined earlier, this may indicate one cause of increased mortality from CHD (Ramezankhani, Azizi, and Hadaegh, 2019).
Index of Multiple Deprivation (IMD)
IMD is an indicator of socioeconomic disadvantage used to identify communities with high levels of deprivation within a geographic area (Qi et al., 2022). For Ward X, this indicator is 54%, indicating that this community performs worse than 46% of other areas in the UK (UK Local Area, 2021). In the breakdown statistics, Ward X performs best on deprivation in education but worst on crime, as shown in Figure 17.
Determinant of Health in Depth
Based on the data analysed earlier, health determinants such as smoking, unemployment, and diabetes must be considered. The detailed community review has shown that these are among the most important for the Ward X population. The unemployment rate in the local population was 4.5% compared to 4.4% in England, and smoking and obesity were identified as critical predictors of diabetes. Among Ward X’s population, 7.4% have diabetes compared to 7.1% in England. These social determinants are caused by several factors, including psychological and physical health problems; they can provoke serious health complications.
The first determinant of health is increased unemployment. For many people, the loss of a job and a steady income can cause psychological health problems. Mamun et al. (2020) underlined that “depression, anxiety disorders, stress, are associated with unemployment due to factors such as increased competition, joblessness, low wages, lack of scopes in practising acquired skills” (p. 1150). In addition, it is noted that a lack of professional employment can lead to feelings of isolation due to a lack of communication and interaction with the community. Financial problems can become a significant barrier to accessing health services, which is reflected in a further deterioration in the health status of the unemployed population. Thus, in addition to mental health, the quality of the population’s physical well-being and quality of life can be significantly reduced.
Against the background of increased stress levels, individuals may resort to addictions such as smoking, which is the following determinant. Research stated that “smoking was a stronger predictor of a long life than wealth or any other social determinants of health” (Heath, 2022). Tobacco addiction significantly reduces well-being, as well as exacerbates the mental characteristics of individuals. Furthermore, their inability to pay for health programmes denies them the opportunity to get qualified help to quit smoking.
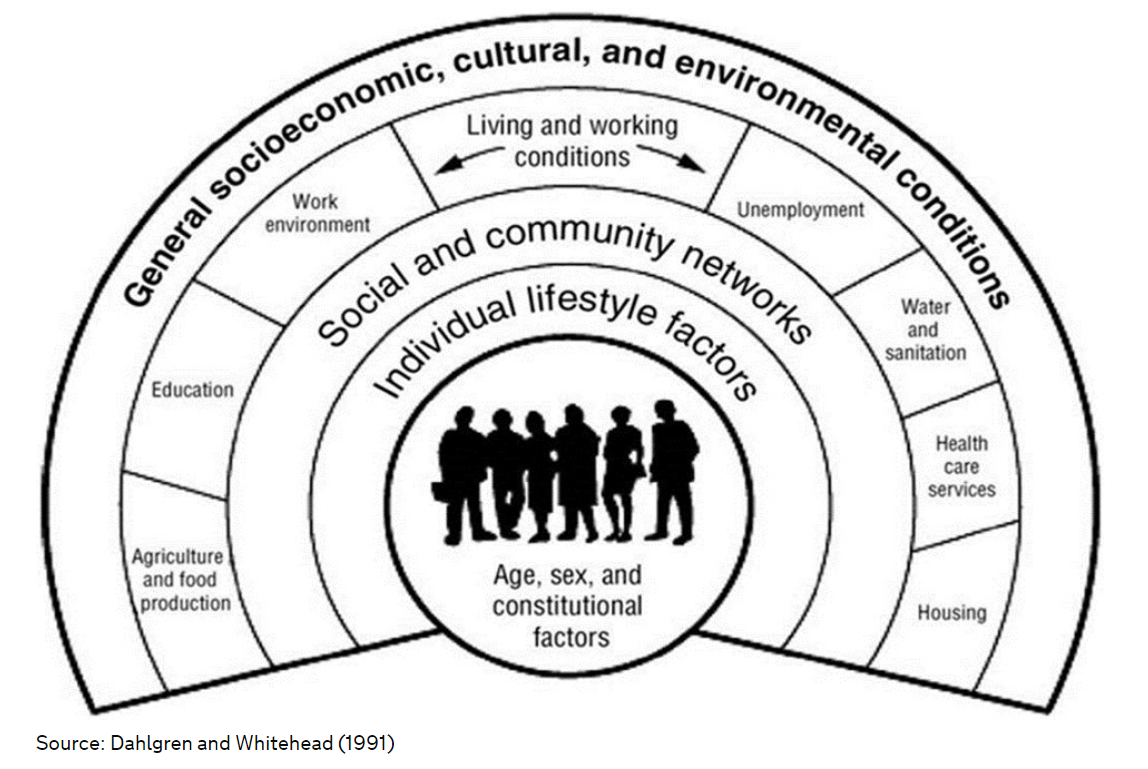
Lack of employment and a commitment to smoking may increase the incidence of diabetes mellitus among the population. This is supported by the fact that these factors place people at risk for this disease, reducing immunity and overall well-being (Mamun et al., 2020). Health services are a critical aspect of social and community networks that can help to prevent this problem (Fig. 18). Thus, the lack of resources and opportunities associated with unemployment contributes to the limited availability of healthcare that would help to reduce the adverse effects.
Becoming unemployed significantly impacts workers’ health, contributing to its consideration as part of the occupational health of Ward X. This is because this circumstance directly affects individuals’ physical and mental health (Mamun et al., 2020). Occupational health professionals can play a decisive role in preventing this societal problem.
The primary approach that can be applied as a solution to this problem is to work with employers in Ward X. These professionals need to ensure that acts are created and enshrined to negotiate the conditions to provide resources for workers during unemployment. Examples of these initiatives could be programmes to provide health services to support psychological and physical well-being. These could include smoking cessation, specialist diabetes care, and counselling for mental health problems caused by a lack of work. Employers can provide access to medical check-ups and provide employees with health insurance. Furthermore, they can provide financial counselling for employees, training programmes, and payments in particularly critical cases.
Moreover, the National Institute for Health and Care Excellence (NICE) has several recommendations to help limit the harmful effects of the determinants discussed and improve public health. Thus, the main one is to reduce unemployment, which is becoming a decisive factor for Ward X (NICE, 2016). A significant part of these recommendations is the application of policies and practices by employers and governments that will help to retain employees and reduce the possibility of job losses. Furthermore, they introduce assistance programmes that support individuals who have lost their jobs. In addition to the necessary counselling, these should include health promotion initiatives such as smoking cessation and diabetes treatment (NICE, 2022).
In considering this topic, attention should be paid to the ethical, legal, and professional issues that can arise when considering the social determinants of health. For example, from a professional perspective, many employers may find investing in support programmes for workers who have lost their jobs challenging. This aspect includes concerns about legal liability.
Thus, not all existing initiatives can cover the care of unemployed individuals. In addition, there may be concerns about the privacy of workers, which relates to the ethical part of the issue in question. This aspect directly affects mental health or financial problems. To limit the impact of the listed indicators, occupational safety and health professionals need to work closely with employers and authorities to develop practical and ethical solutions.
Finally, social determinants of health, such as unemployment, have a direct impact on the further development of issues such as smoking and diabetes. These are highly detrimental to the well-being of the Ward X population and require the close attention of employers and government bodies. The NICE identifies recommendations that can improve the situation for Ward X, which involve health and safety professionals working with employers to develop practical and ethical solutions.
Recommendations for Practice
Based on the critical analysis and review of Ward X, the following data-driven recommendations can be applied to the community to improve public health, considering the determinants discussed.
- Increase patient access to information resources for diabetes education and management; this could be implemented through classrooms.
- Initiate and support smoking cessation programmes, with particular attention to cultural sensitivities and appropriate resources for ethnic minorities.
- Authorities in the region should increase access to training and employment services to reduce unemployment and increase economic stability.
- Authorities in the region are advised to expand access to training and employment services to lower unemployment and strengthen economic stability.
- Maximise access to healthy eating and physical activity resources, particularly in congregate settings, including the local protected park.
- Maximise clinical access to professional preventive care and education of the Ward X community on cardiovascular health, with particular attention to risk factors such as smoking and obesity. Specific areas for implementing this recommendation include health check-ups, socio-advertising campaigns, and public health exhibitions and fairs.
- Training and information programmes should address poorly educated populations and language barriers.
- Continue to collect and evaluate data, including using technology and AI, as most of the data for Ward X was relevant for 2011. Particular emphasis should be placed on the following:
- CHD mortality rates in the region.
- The rate of unemployment in the region.
- Level of cigarette smoking.
- Level of obesity (child and adult).
- Rate of diabetes incidence.
- Access to health services.
- Use of smoking cessation programmes and resources for diabetes.
- Impact of information resources on perceptions of health (via surveys).
- Impact of information resources on health (through health data analytics).
- Data on transport accessibility.
- Data on environmental hazards, including real-time environmental monitoring of pollution.
Conclusion
This paper has reviewed and critically analysed the real community of Ward X, Coventry, UK, whose name has been changed for privacy reasons. It was found that Ward X, at least according to 2011 data, faces several severe public health challenges, including increased mortality from CHD, high rates of unemployment, smoking, obesity, and diabetes compared to the UK national average. To address these challenges, it is essential to implement preventative and proactive public health actions that aim to increase access to training and employment services, informative education, cessation programmes, and the adoption of healthy lifestyles. Particular attention should be paid to ethnic minorities who are vulnerable to Ward X. Tracking the implementation of these recommendations by obtaining real-time data and analysing them using modern technology will help to assess the effectiveness of interventions and make necessary adjustments, thus improving the health agenda of the region.
Reference List
Bhaumik, S., et al. (2020) ‘Community health workers for pandemic response: a rapid evidence synthesis’, BMJ Global Health, 5(6), pp. 1-20.
Bombak, A.E., et al. (2020) ‘A systematic search and critical thematic, narrative review of lifestyle interventions for the prevention and management of diabetes’, Critical Public Health, 30(1), pp. 103-114.
Buettner-Schmidt, K., Miller, D.R. and Maack, B. (2019) ‘Disparities in rural tobacco use, smoke-free policies, and tobacco taxes’, Western Journal of Nursing Research, 41(8), pp. 1184-1202.
CCC (2022) Wyken. Web.
Chapter 6: social determinants of health (2017) Web.
CityPopulation (2022a) Wyken. Web.
CityPopulation (2022b) United Kingdom: major cities in England. Web.
Dawes, D.E. (2020) The political determinants of health. Baltimore: Johns Hopkins University Press.
de Souza, N. (2022) ‘Nightmare’ gridlock fears as new Coventry waste site opens next to busy primary school. Web.
Eurostat (2021) Archive: urban-rural typology. Web.
Hamidi, S. and Hamidi, I. (2021) ‘Subway ridership, crowding, or population density: determinants of COVID-19 infection rates in New York City’, American Journal of Preventive Medicine, 60(5), pp. 614-620.
Heath, S. (2022) Smoking trumps other social determinants of health impacting mortality. Web.
Hooper, M.W., Nápoles, A.M. and Pérez-Stable, E.J. (2020) ‘COVID-19 and racial/ethnic disparities’, Jama, 323(24), pp. 2466-2467.
Mamun, M.A., et al. (2020) ‘Financial threat, hardship and distress predict depression, anxiety and stress among the unemployed youths: a Bangladeshi multi-city study’, Journal of Affective Disorders, 276, pp. 1149-1158.
Mauvais-Jarvis, F., et al. (2020) ‘Sex and gender: modifiers of health, disease, and medicine’, The Lancet, 396(10250), pp. 565-582.
NHS (2021) AHP students in public health settings – background. Web.
NICE (2016) Individual research recommendation details. Web.
NICE (2022) Type 2 diabetes in adults: management. Web.
Nomis (2011a) Wyken ward (as of 2011). Web.
Nomis (2011b) England country. Web.
OGL (2023) River Sowe at Wyken and Stoke, Coventry flood warning area. Web.
OGL (n.d.) What qualification levels mean. Web.
OGL (n.d.) What qualification levels mean. Web.
OHID (2023) National General Practice profiles. Web.
ONS (2021) National life tables – life expectancy in the UK: 2018 to 2020. Web.
Qi, X., et al. (2022) ‘Index of multiple deprivation contributed to common psychiatric disorders: a systematic review and comprehensive analysis’, Neuroscience & Biobehavioral Reviews, 140, pp. 1-11.
Qpzm. (2021). Wyken demographics (Coventry, England). Web.
Ramezankhani, A., Azizi, F. and Hadaegh, F. (2019) ‘Associations of marital status with diabetes, hypertension, cardiovascular disease and all-cause mortality: a long-term follow-up study’, PloS One, 14(4), pp. 1-15.
Sá, F. (2020) Socioeconomic determinants of Covid-19 infections and mortality: evidence from England and Wales. Web.
Sarangi, A., Kim, D. and Rafael, J. (2022) ‘The mental health impact of work from home: a literature review’, The Southwest Respiratory and Critical Care Chronicles, 10(45), pp. 10-18.
Schork, N.J. (2019) ‘Artificial intelligence and personalized medicine’, in Von Hoff, D. D. and Han, H. (eds.) Precision medicine in cancer therapy. Cham: Springer, pp. 265-283.
Stømer, U.E., et al. (2019) ‘A cross‐sectional study of health literacy in patients with chronic kidney disease: associations with demographic and clinical variables’, Nursing Open, 6(4), pp. 1481-1490.
UK Census Data (2022a) Wyken E00049129. Web.
UK Census Data (2022b) Wyken. Web.
UK Census Data (2022c) England. Web.
UK Local Area (2021) Wyken Coventry 019D. Web.
US (2021) Introduction to research skills. Web.
Varbes (2023) House prices in Ansty Road, Wyken, Coventry, CV2. Web.
Vinsights (2021) Wyken, Coventry: ward level demographics composition covering the last two census. Web.
Zoopla (2021) How home values compare by floorspace. Web.
